Not very well actually.
First some definitions from the CDC:
Clinical Description of Acute HCV
“An acute illness with a discrete onset of any sign or symptom* consistent with acute viral hepatitis (e.g., fever, headache, malaise, anorexia, nausea, vomiting, diarrhea, and abdominal pain), and either a) jaundice, or b) elevated serum alanine aminotransferase (ALT) levels >400IU/L.
*A documented negative HCV antibody laboratory test result followed within 6 months by a positive test (as described in the laboratory criteria for diagnosis) result does not require an acute clinical presentation to meet the surveillance case definition.”
In other words, they write elsewhere: “No symptoms are required.”
Laboratory Criteria for Diagnosis
“One or more of the following three criteria:
- Antibodies to hepatitis C virus (anti-HCV) screening-test-positive with a signal to cut-off ratio predictive of a true positive as determined for the particular assay as defined by CDC. (URL for the signal to cut-off ratios:http://www.cdc.gov/hepatitis/HCV/LabTesting.htm), OR
- Hepatitis C Virus Recombinant Immunoblot Assay (HCV RIBA) positive, OR
- Nucleic Acid Test (NAT) for HCV RNA positive (including qualitative, quantitative or genotype testing)
AND, if done meets the following two criteria:
Absence of IgM antibody to hepatitis A virus (if done) (IgM anti-HAV),
AND Absence of IgM antibody to hepatitis B core antigen (if done) (IgM anti-HBc)”
Case Classification: Confirmed
“A case that meets the clinical case definition, is laboratory confirmed, and is not known to have chronic hepatitis C.”
The CDC states that “no laboratory distinction can be made between acute and chronic (past or present) HCV infection,” on page 8 of a report: Viral Hepatitis Surveillance, United States, 2010 by the CDC. Chronic HCV is only diagnosed after repeat testing.
Do these fuzzy definitions call into question many of the VA’s own fuzzy analyses of acute HCV infections?
National Notifiable Disease Surveillance System (NNDSS) collects hepatitis C data weekly. The numbers on newly confirmed cases of acute symptomatic HCV remain spotty so they use mathematical modeling to make estimates.
“…for each new reported HCV symptomatic infection 20.0 new HCV infections (of which 3.3 and 16.7 cases were symptomatic and asymptomatic, respectively) are estimated to occur in the general population.”
The need to estimate isn’t surprising given that acute symptoms such as fever, headache, malaise, nausea etc.. are not only common to many illnesses even it they occured often.
The interactive CDC NCHHSTP Atlas good way to learn about acute Hepatitis C infections. There is a video tutorial to view. Click query, choose acute hep c from drop down menu, click update map button. To see yearly figures from reporting states, hover your curser over a bar in the National Data table. For 2010, I see 850 reported.
Multiply 850 x 20 = 17,000 estimated acute hep cases that were not diagnosed 2010.
(Click image to go to Atlas.)

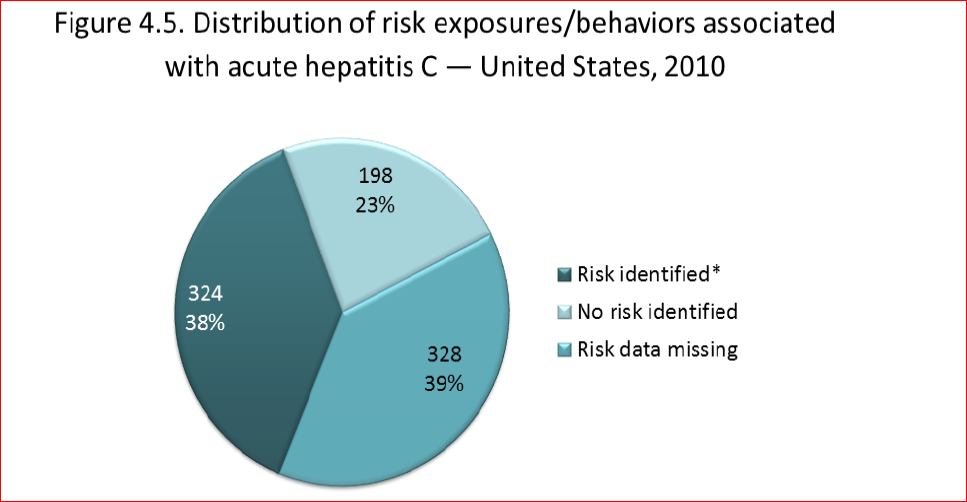
One view of the CDC Altas of 2010 acute Hep C cases
Of the 850 (mainly young people), a pie chart is offered in the above report.
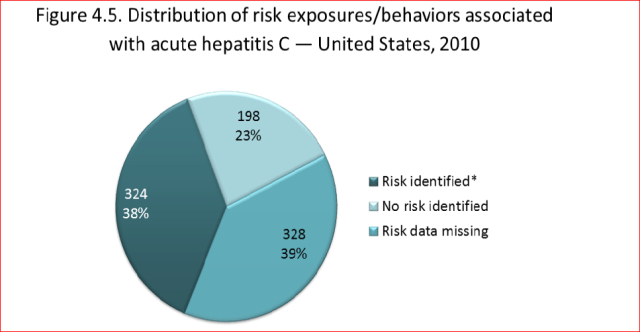
Of the 38% who reported a recent risk factor, they lumped together the following exposures and behaviors (I changed the order):
1. underwent surgery 2. A percutaneous injury 3. A blood transfusion 4. hemodialysis/kidney transplant 5. occupational blood exposure 6. sleeping around 7. MSM (assume unprotected anal sex) 8. sex with hcv partner (or suspected hcv) 9. IV drug use.
Why would they even ask about blood transfusions? Isn’t HCV inactivated in plasma products in the US nowadays?
Also, some of these newly diagnosed “acute” patients had to be hospitalized and some died.
Well, it’s a jumble. On Monday, you’re an acute HCV patient; on Wedsnesday, you’re a chronic HCV patient. No matter how you look at it, you’re in big trouble.
But we need to pay attention to the CDC and its new KNOW MORE HEPATITIS educational campaign. It may be a game changer and will help veterans as information gets out.

ANYONE born from 1945-1965 get tested for hepatitis C