
And the envelope, please. From Carrie Stiffler, this week’s winner is….
You find some funny stuff on the Facepage.
And the envelope, please. From Carrie Stiffler, this week’s winner is….
You find some funny stuff on the Facepage.
I suspected this was going to hit the books in record time and I was right. Barely a week later following Walker, we are seeing it being cited. Seriously. A week? When my BVA decision was announced in 1992, no one mentioned Wilson, Shafrath, Bagby and a host of other Vets whose jurisprudence bore a striking resemblance to mine. Yet here mandate ink is barely dry and decisions that were months in the offing suddenly are sporting this new law. Seriously. Mr. Walker still has an opportunity to appeal this to the Supreme Court so I find it odd that this is now dyed in the wool precedence.
You heard it here. You will remember for years following this post that we said here the implications of Walker are going to rock the Vets world. This is a single-judge decision but is just the sound of a juggernaut warming up.
One thing is apparent. The landlines of the good Drs Bash and Ellis will be ringing off the hook. I have an idea. Let’s get some venture capital together and set up a corporation like unto QTC Medical Services Inc. Our service will provide low-cost medical nexus letters from a stable of participating doctors schooled in the appropriate sciences. If we wished to be political about it, we could do a means test and charge rich guys enough to make them blow Starbucks® through their nose. They, in turn, could finance pro bono cases with the exorbitant fees. The client (Veteran) signs an agreement wherein he agrees to pay the amount due upon the grant of the claim. The doctor will be available to rebut anything VA uses to deny. The nexus will be ironclad and warrantied based on the truthfulness of the claimant. If the Veteran submits a fraudulent claim, his nexus bill would still be due and owing to said corporation.
I vote for Legalnexus.com

Legalnexus.com warranties this nexus as viable for all 56 VAROs and the AMC with certain restrictions. Dealer Prep and destination fees not included. Does not include energy surcharge or travel time to and fro from (your VARO here) to Washington, DC. legalnexus.com reserves the right to refuse service to those with no shoes or shirts.
To view Mr. McMillan’s unhappy visit to Indiana Ave. click here and then click on number 17 which is Mr McMillan- case number 11-3003. Walker was decided February 21st. Mr McMillan suffered this ignominious treatment on the 28th- a mere seven days later. Which means either justice is incredibly speedy at the CAVC or they cut and pasted a new ending to the story. Considering he would have prevailed sans Walker, can anyone see a different outcome other than a win?
This is, as I have pointed out, merely the beginning of an avalanche of denials. What concerns us all is how many of you will be divested of your ratings for prior adjudications based on 38 CFR § 3.303(b). I shudder to think how many of you are on the cusp of VA CUEing themselves. If it only affected one hundred of you, I wouldn’t sound the alarm quite so stridently. Since I know VA better than most, I fully expect them to fire up the computers and begin searching for the .pdfs with 3.303(b). Keep in mind, too, that VA is now in the process of scanning millions of records into the system for the new VBMS.
Backlog? you don’t know the half of it. 2015 and 125 day adjudications just flew out the window. Whole TIGER teams of Challenge -trained RVSRs fresh out of the Academy with Lean Six Sigma black belts and Kaizen training are going to be on this like white on rice, Grasshopper. The savings from this could potentially fund the next five HR conferences on the French Riviera with bonus money left over. Karaoke en Français anyone?
This Congressman serves on the Veterans’ Affairs Committee and may be a friend.
Congressman Jeff Denham represents the 10th District of California in the U.S. House of Representatives. His district includes all of Stanislaus County and part of San Joaquin County. He was first elected to Congress in 2010, and is currently serving a second term in the 113th Congress.
Rep. Denham’s public service career began with the U.S. Air Force, where he served for 16 years between active duty and reserve status. He fought in Operation Desert Storm and Operation Restore Hope in Iraq and Somalia, respectively.

VA’s latest publication on why we are in deep doo-doo is intriguing. The backlog has more excuses than Carter has pills. I know that sounds old fashioned but this needs no tortured explanation. All the flag waving is merely a distraction.
My daddy said a bunch of things in the course of his life. Most were non-judgmental. They were simply observations about human nature. One that stands out in my mind is that the more a body (or a government agency) explains how they got into a fix, the true magnitude of the problem is inevitably being marginalized.
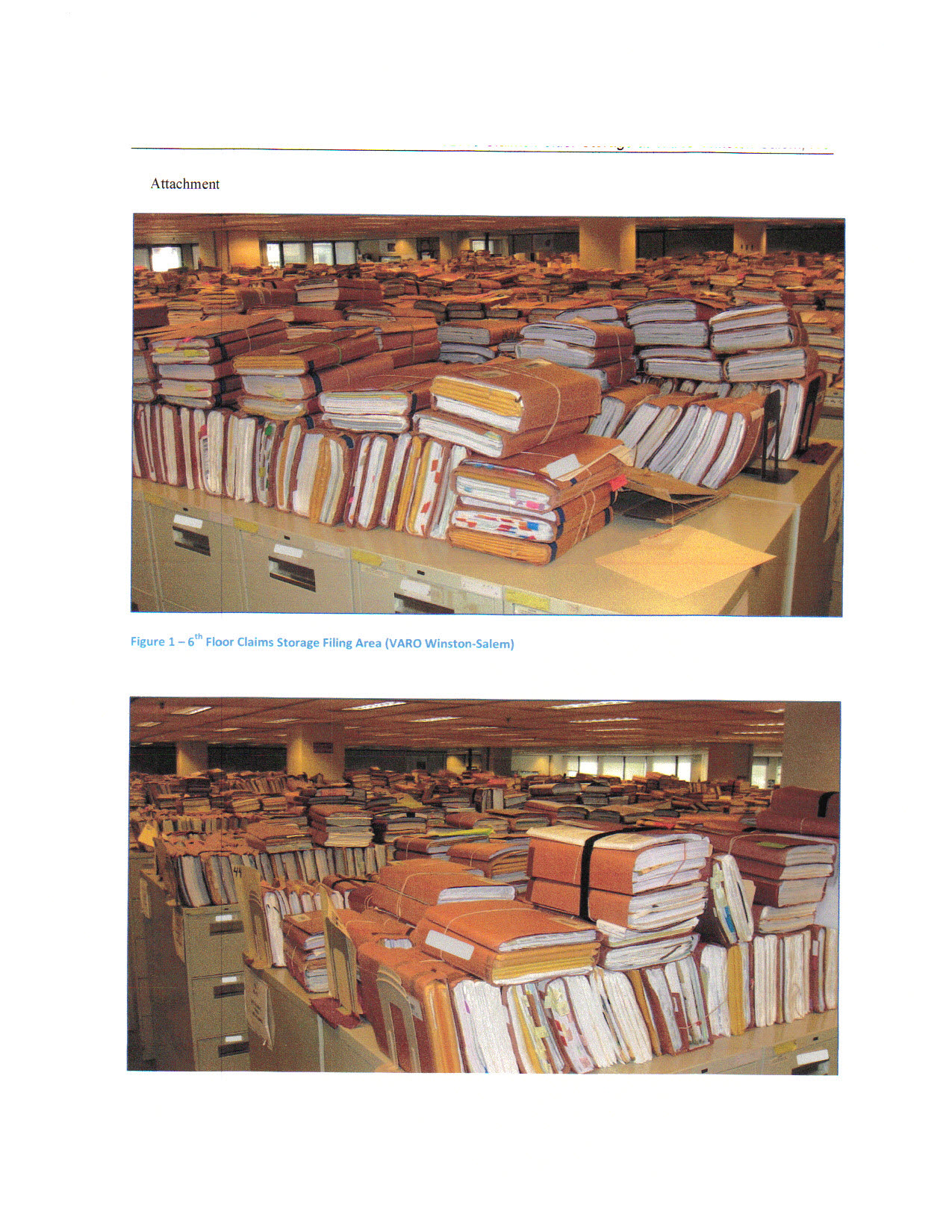
VA attempts to change their story line and spends beaucoup bucks on PR in the process. In 2009, this was simply a matter of hiring more worker bees and training them. In 2010, we were eagerly awaiting the completion of their training and subsequent deployment. Suddenly, in 2011, we discovered the enormity of the paper file tsunami. In order to go barefoot with VBMS, we had to scan the equivalent, pulp-wise, of all the trees ever cut down in America since 1776. My guess was someone in authority went up to the sixth floor of the Winston Salem Cigarette RO and noticed all the files stacked up in 1994. He multiplied that by 57 ROs ( I count the AMC black hole as one) and it dawned on him that it was going to take every reproduction company in America about 10 years to scan, collate and make them .PDF word-searchable based solely on the numbers of Vets back then. The enormity of the problem was so depressing, he went back downstairs and elaborated. They promoted him for being such a far thinker and then did nothing.
Hand-written records are not, nor ever will be, word-searchable, so VBMS still is no panacea. This is the ugly stepsister VA hasn’t even disclosed yet. That shoe will fall in 2015 when they can’t possibly meet Revered Leader’s 125-day/98% accuracy goals. In short, failure is once again built in with ultimate deniability. All the Vietnam Vets through the late 80s, with their hand-written STRs are hitting the wall and they all have illegible, handwritten records that demand a sleuth with a magnifying glass. The current training for VA examiners no longer includes the curriculum. This means the records, for all intents and purposes, are not viable evidence unless a Veteran can provide a translation. That does not guarantee VA’s finest will accept it. Much like the inhabitants in the next state over from Missouri, they’ll see it when they believe it, and not a minute sooner.
The VA appears as though they live in faery tale land. Either they are convinced in their own minds that what they write for us is true or they are smoking something better than what the medical marijuana salesmen are hawking.
Silly rabbit. Trix are for Vets. All this time we were using the wrong name for it. Calling it Inventory or backlog is immaterial in that it still doesn’t explain what VA called the identical problem in 1992 or 2008. The delay has always been there regardless of what or how one characterizes it. This didn’t just materialize out of thin air after September 11th, 2001 but now we are expected to believe if we magically add up the “inventory” and the “backlog”, we can better define the problem and solve it. Only in D.C would properly naming a defect simultaneously present the cure for it. That only works in Hollywood movies.
VA has always been a past master at obfuscating, going off on a perpendicular tack or manufacturing a straw man and pointing to it as the sole reason why they are unable to perform. This manifesto is no different. It subtly diverts attention away from their centuries of wastefulness, carpetbagging and featherbedding.
Apparently VA has never noticed the correlation between armed conflict and casualties. You would think that if this is all they do for a living, the Undersecretary for Job Security would sit up one day down at Vermin Ave. and say ” Mikey. Hey, Mikey. Did you know that every time they have a war like Iraqistan a whole bunch of people start sending in claims? I mean, like way more than a normal amount? This is like, totally awesome. It explains the backlog, dude. Manna, I’mma gonna getta bo-nusssss.” (sung liltingly). The fallout of WW2 must have also come as a big surprise sixty eight years ago. In fact, they may not have even noticed the blip of Korea or Vietnam on their claims radar if they are that dense.
The fact that they feel this needs to be restated indicates somewhere, a village is missing it’s idiot. Who did they write this for? Veterans Service Representatives? Here the VA attempts to blame the internet…
Perhaps we should add that when they created a neetsy keen thing called the Benefits Portal (Ebenefits), this became inevitable. Are they now conflusticated that Vets actually avail themselves of this technology? The military washes their hands of us like Pontius Pilate when we separate. They encourage Vets to file and wonder of wonders- they do. Now VA cannot fathom why they are filing so many claims. All that is finally covered in this missive.
Gee, where’d you park the squad car, Dick Tracy? So we now have an ample description of what caused the problem. Veterans appear to be at fault for filing in such large numbers and with such enormous numbers of ills. The military (read Bush 41& 43) is also a culprit for being so bellicose and warlike. And lastly, the American populace is indicted for being greedy and crashing the economy. In sum, everyone but the VA was instrumental in causing this perfect storm. They are merely trying to keep their heads above water and cope with it.
To add to this cacophony of dysfunctionalism, we are beginning to find out that someone is stretching the truth at the DVA. We had hoped to see an eventual melding of the two dissimilar computer systems of DoD and VA into one seamless, integrated network where a Vet could separate from service and file electronically with VA as necessary. His medical records, in this more perfect world, would simply pop up and populate a new Form 21-526 (e) (e for electronic) when he notified VA he was ready. Even better yet, they would be “pre-filed” before separation and the Vet would begin drawing his VA compensation on Day One after walking off base. Not. Panetta and Dear Revered Leader weren’t even on the same page recently at a joint Dog and Pony show. Both spoke but the bubbles they were blowing weren’t the same size and color. It didn’t faze them a bit that their comments were mutually exclusive and contradicted one another. Onward through the fog. More computers. More money. More personnel. More time. More. More. More.
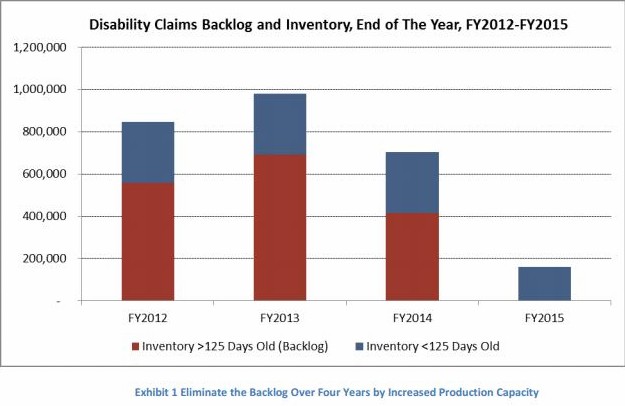
One thing that catches my eye and should be cause for alarm is the straw man mentioned above. He is going to be the fall guy when things don’t pan out. The foundation is being carefully constructed and cardboard cutouts are being erected to appear authentic. The following graph and explanation are an example. Notice everything is couched in ” This is what is supposed to happen” or “We foresee a gradual…”. Planning at VA has been non-existent for centuries and is a spurious combination of “Oh, shit! When did that happen?” followed by lots of “Perhaps they won’t notice” or “I hope this doesn’t affect our tee time.”.

Take-down chart? This sounds like a Swat maneuver. Col. (Brevet Maj. General) George Custer had a chart similar to this in his hat when found above Minneconjou Ford. It carefully detailed what the Indians were planning and the adequacy of his response. I’m sure the captain of the Titanic had a similar one threading a path through all the open sea ice infesting the Northern Atlantic every April. The point I’m trying to make is that VA’s suppositions are manufactured much like a billiards game. Wait until the ball quits rolling to make a decision. Nothing is committed to paper until failure is imminent. At that time, a new, improved game plan is instituted that will carry the day. Each and every plan fails but that does not dull the enthusiasm of the planners. They dutifully return to their chalkboards and start drawing anew. No mention is made of failure or poor planning. No bonuses are relinquished for failures of judgement. Quite the contrary. Even larger bonuses are dangled in front of them and exhortations to stem the tide are shouted louder. Congress instituted the VJRA in 1989 to fix this. Old habits die hard. Really old habits are immortal and refuse to succumb at the VA.
VA resorted to acronyms several years ago to enunciate how they were taking the backlog fight into the field. We’ve reported some and invented a few humorous ones of our own to make our point that catchy phrases sell cars and potato chips. They do not change reality. Challenge Training is all well and fine in teaching RVSRs the mechanics of the claims process. If you’re still driving a paper model T, the chasm is too wide to ford and no amount of training is going to bridge it. Which leads us to the miracle of technology. Would that this were the case.
VA belatedly launched their VBMS plan in 2012 as a last ditch effort to modernize. They took 4 (four) (quatre) (see) VAROs and said that henceforth all claims would be done electronically. First, a company had to be located on short notice to start scanning in the Vet’s records. Next, the .PDF format had to be word searchable or all they had was an incredibly small filing cabinet where the Vet’s records couldn’t get lost or misplaced. Whoa, hoss. Don’t bet on that one yet. They probably haven’t right clicked and made a copy. VA has a storied history for losing things. Finally, the new electronic file had to be organized uniformly such that each VSR could access them and find everything in the same place.
Think left flap, center flap and right flap. For those of you uninitiated, a C-file is a file folder that opens with three parts and two folds. Take a piece of paper and fold it like a letter into three equal components and you’ll get the picture. Currently the left flap has to do with dependency, wives, kids, etc. The center flap is all about compensation. The right is VR&E, VA loans and other entitlements. If I have the right and left flaps reversed, excuse me. My brain is getting defective.
After collating and scanning, the organization was next. Following that, VSRs were expected to go online into the bowels of the VBMS and use it to manufacture ratings. Who would have thought that the four VAROs would all try to access the national VBMS database simultaneously during daylight hours? The VBMS promptly became the VBSM and crashed. All the VASEC’s horses and all the VASEC’s men couldn’t put VBMS back together again. Soon it was back to the hitting the books with the old analog pencil and paper. VA is now claiming that they have no less that 12 VAROs VBMS operational. As with all that wanders out of the mouths of the VA talking heads, the definition of “operational” is key to understanding this. Here’s the mantra posted on all the bulletin boards of the new VBMS-equipped VAROS…
This was lifted from Bernie Madoff’s game plan. It also bears a striking resemblance to the expensive Dave Del Dotto Cash Flow System brochure (and cassette tapes) I bought back in the eighties. It sounds good on paper. VA calls that the “paper view” as in “We designed this on paper and it appears as though it will fly”. The numerous IT contractors asked to bid on this hodge podge of new ideas refer to it as “pay-per-view” as in “Sure, we’ll build it for you just like you drew it here. Unfortunately it won’t work the way you drew it. When you come back with a change order, we’ll build that version so you can pay to view it as well.”
What I think VA fails to comprehend is that their IT gurus are the ones who clung to the paper files systems for decades past when even their very own contemporaries in government realized its neanderthal potential. Now, like newbies wanting to have the shiny new skateboard on the block, they are grasping at anything to appear more modern and knowledgeable. As we all know, you let the geeks figure this out. Give them the parameters of what you need, the stringent mission needs and get out of the way. The worst thing you can do is hire a bunch of your own talking heads, none of whom speak the same language, and turn them loose on a project of this enormity. They’ll tell you anything you want to hear if you’re cutting the paycheck.
VA has been building a Tower of Babel for the last few years. In construction, we have an apt term- Eventually you have to shoot the engineers and begin production. VA cannot bring itself to do this. They endlessly continue to tamper with the model and commit inadequate resources to any one facet of it. Thus you have no national infrastructure set up to scan the C-files but just a few local yokels with no instructions on the parameters and needs. Each varies from RO to RO with no uniformity built in. Computer servers haven’t been set up because no one has allocated sufficient funds for a massive server farm somewhere to accommodate it (yet). Nevertheless, VA has put in place a plethora of cute acronyms to describe what will happen in this new idyllic world they are creating. It’s like taking your Erector Set® down to the World Trade Center and asking “Where do I set up?”
Allow me to pluck from some of the choice phrases that so richly adorn this document.
I believe these are Karaoke terms. Either that or they are Yoga positions. “Targets of opportunity” leads me to believe former military planners have their fingerprints all over this.
Simply read, VA was too cheap to go out and hire think tanks to unravel this. Instead, they installed “structured mechanisms” called “suggestion boxes” in VARO rating rooms, VSOs and VFW bars. Veterans from Rio Linda can be excused for misreading the spelling of “stakeholders” and demanding grass-fed beef with their claims.
This is one of the few true statements in the document. They did do this. Now your denial letter is couched in fewer keystrokes. Of course, it’s computer generated so it really didn’t speed up anything ratings-wise. The form now simply says “We made a decision-No!” The beauty of this is manifold. By using denial as the default setting more broadly and rapidly, productivity will appear to go through the roof. When the chickens come home to roost from remands two and three years down the road, a new backlog will begin. VA will deal with that when they get there. Anything post-2015 is not programmed in because they haven’t ever faced that eventuality yet.
Whoever dreamed this one up got the “Let them eat cake” award. Imagine making a claimant go out and get everything needed to assess his claim. VA does nothing. Once assembled, the rater simply makes his/her decision based on what the M21 spits out (denial) and sends it up for a signature and the steno pool. What could be simpler? This should, by rights, leave the raters with ample time to brush up on their upcoming Karaoke competition in Orlando this summer. That it will make severe inroads into the backlog is without question. Duty to assist, as an obligation, will fall into disuse and be supplanted by “Dude, you didn’t give me a FDC. I can’t rate it.”
And then there’s the dilemma of scanning I mentioned. VA glosses over this with another acronym (VCIP) that blithely ignores the 800 lb. gorilla with handwritten records. They gleefully point out that they’ll be up and running on this to the tune of 70 million images a month from 5. Really? My C-file contained 3.517 individual sheets of paper to scan. My attorney asked for it on the 26th day of June 2012. We received them in October. This was mandated by the CAVC to be done within sixty days of the filing of the Notice of Appeal. VA must not have gotten that email.
What VA fails to reveal is that the VCIP contractors came back to the VA and started asking questions almost immediately about how they (VA) wanted the scans organized. The next burning question was what to do with all the hand-written medrecs. Each contractor at the four original VBMS test VAROs were given conflicting instructions. As for the handwritten ones, VSRs are instructed to revert back to analog on them. So, at best, newer “round peg” claims will fit into the round hole whereas older “square peg” handwritten claims will suffer the same slow “inventory” semantic or is it “backlog”?
There is no simple solution to this. VA should have begun it in the 1990s when they had the foresight to go to the VISTA system employed by their VHA. They didn’t and now they are paying the piper dearly. It wouldn’t be so disagreeable if VA would just own it and get ‘er done. Instead, they erect the staging and call the media for grandiose soundbite news about how they are winning the war on the backlog. The more they try to convince me that they can see the light at the end of the tunnel in 2015 convinces me of my father’s observations. They haven’t a clue what they are about but they can sure talk a blue streak about how to fix it.
How about this one? Count them. No less than six acronyms to cut the Gordian knot. At this rate, by 2015, VSRs will be accosting you in supermarkets or Costco and begging you to file claims because they are under-employed. In fact, they’ll be researching our e-records desperately in hopes of finding some entitlement they overlooked in years past that is due and owing. After the Fed. Circuit’s Walker decision, you can pretty much count on it.
Well shoot, pilgrims. Problem solved. Them fellers down at Vermont Avenue have this all sewn up. Good thing too. This was threatening to have tremendous repercussions on Veterans as most know. Now, with the insertion of a bunch of letter combinations, all our worries have been addressed. VA has come back down from the mountain with the sacred tablets. They have drawn colorful pictures that even Dick and Jane can digest. One minor problem seems to be cropping up. A lot of the DBQs are about as long as a 21-526 and many private doctors are demanding money to sit down and fill them out. Who woulda thunk it?
Here’s the one I like.
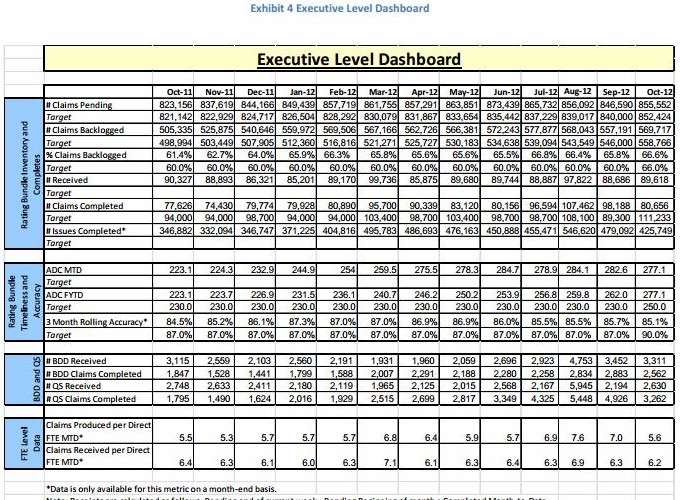
Check out the three month rolling accuracy with the asterisk beside it. Does anyone find it odd that the data is only “available for this metric on a month-end basis”? How is it they can project these mythic percentages? From my readings of the Veterans Benefits Manual from Lexis Nexus, it categorically pokes a rather large hole in their data. Based entirely on the outcome of judicial proceedings, it has been determined that VA is in error at least 60% of the time in their decisions. If this wasn’t cause for alarm, it doesn’t even encompass the vast quantity of JMRs where VA admits no wrongdoing and asks for either a do over or a settlement on the Courthouse steps before you enter. Those “errors” never enter the system as hard statistics and are lost. If included, it would point to an error rate of 70% which is appalling. VA can’t or won’t explain the disparity between their data and documented judicial percentages.
Why is there no hue or cry when a government agency publishes a document rife with propaganda and lies? How can it be that this will represent the true state of affairs? Do the VSOs of America subscribe to this pablum and swallow it uncontested? Is there no one who will stand and cry foul? Do we have to wait until 2015 to find out (once again) that but for a glitch in statistics, all the carefully laid plans were for naught ?
Always remember that when someone dumbs down the explanation for the problem and writes it out, it will probably state the obvious like ‘The sun rises in the east in the morning and sets in the west in the evening. This explains that dark stuff in between.”
Try this one on.
So near but yet so far.

global HCV prevalence click
Information about HCV on the CDC website is evolving albeit slowly.
Click the map for a larger view. Imagine that all veterans with HCV (resolved or active infections) were isolated together in their own country. They’d have to provide a different and darker legend color because a prevalence of 2.9% is not descriptive enough illustrate the magnitude of HCV in the veteran population. In fact, the HCV endemic all the countries should be marked with a different color.
According to 2006-2007 research (click table for larger image), among the HCV endemic countries are: Egypt (18%); Rwanda (17%); Cameroon (17%); Burundi (11%); Bolivia (11%); Guinea (11%); Mongolia (11%).
But medium/high risk countries are countries that have a prevelance of HCV over 2% according to these researchers’ references.
Map Source:
In my opinion, there is little enthusiasm or concern about the domestic or global HCV crisis from the CDC’s leadership.
I don’t know how a Twitter chat works but this is an opportunity to ask questions about HCV testing, blood safety, safe injections, within the context of global health and Haiti. I do know that HIV is prevalent in Haiti.
http://www.cdc.gov/features/twitterchat/
https://twitter.com/DrFriedenCDC
Dr. Frieden will be joined by an expert from CDC’s Center for Global Health to discuss the public health achievements in Haiti over the past three years, and answer your questions about how CDC’s work around the world protects the American people from health threats, wherever they arise.
When:
Thursday, February 28th, 1:00-2:00PM EST
Join the conversation:
Follow Dr. Frieden on Twitter @DrFriedenCDC![]() and use the hashtag #CDCchat to participate.
and use the hashtag #CDCchat to participate.
An official history from the Army provides some intriguing information about blood supplies that may provide hints about why certain HCV strains are prevalent in Vietnam veterans–and why hepatitis C is endemic in Vietnam veterans.
Source of the quotes below: http://history.amedd.army.mil/booksdocs/vietnam/medicalsupport/chapter9.html
First, the need for blood:
“As troop strength grew and combat casualties increased, the task of distributing whole blood, plasma, and related products in South Vietnam developed into the largest blood distribution system ever undertaken by a single organization.”
“…requirements for whole blood would climb slowly but steadily from less than 100 units per month in 1965 to 8,000 units by February 1966, skyrocket to more than 30,000 units per month by 1968, peak at 38,000 units in February 1969, and fall rapidly to less than 15,000 units by mid-1970.”
At first, blood sources came from Asian donors and military donors.
“The primary source for whole blood used in South Vietnam until July 1966 was the 406th Medical Laboratory in Japan. Mobile bleeding teams were dispatched from the laboratory to donor resources in Japan, Korea, Okinawa, and Taiwan. A very valuable donor resource was found in the Yokosuka Naval Base when the Pacific fleet came in, and reserve donor resources also existed in Hawaii, Guam, and the Philippines. With vigorous command support and the dedicated work of blood-drawing teams, supply kept pace with demand until June 1966. Blood collections in PACOM rose from 201 units in January 1965 to 7,426 in January 1966 and 12,984 in June 1966.”
Then came a big change. Blood was collected by 42 donor U. S. military centers designated by The Surgeons General of the Army, Navy, and Air Force and shipped by air to Asia.
Only American military personnel (and military-related persons) donate blood to American forces in Vietnam.
“For the first time in U.S. military history, every unit of whole blood used to support the war was donated free of charge by military personnel, their dependents, and civilians employed at military installations.
Donors were not motivated by profit. No high-pressure advertising programs were permitted, yet nearly a million and a half volunteers gave blood. Not once was it necessary to initiate contracts for blood to be supplied by the American Red Cross or the American Association of Blood Banks. Even in the most difficult times, when blood requirements reached 38,000 units a month, the civilian blood collection system was not upset by the additional military requirements to support an ongoing war.”
1. First Asian blood > transfused into injured American forces in Vietnam.
2. Then only American military personnel blood (and related persons)> transfused into injured American forces in Vietnam.
My lay theory: Transfusion-based chains of blood-borne infections occurred because after 1966, the system became, please excuse this word, incestuous, since no military-related civilians were donors. It was a closed system.

Vietnam battlefield transfusion in 1967

Member Carla writes and says “my husband has lost the use of his creative organ for all intents and purposes. They attribute this to his DM2. He was also blinded in one eye from shell fragments during a mortar attack in Vietnam during his tour. They were paying him Special Monthly Compensation (SMC) K. My question is simple. Can he have two K ratings at the same time? Our VSO says no and won’t file us for it. What’s the law?”
Well, Carla. Ratings accrue from 0% up to 100%. Certain parts and pieces we’re missing are remunerated slightly differently beyond 100%. Finally, if we are missing too many or some go bad, we advance up the ladder. SMC is awarded for “quality of life” issues above and beyond 100% disability. Up until 1961, only those Vets who had served in a time of war qualified. Here are the SMC compensation dollar amount tables.
https://www.va.gov/disability/compensation-rates/special-monthly-compensation-rates/
At the end, when we are on our deathbed, we’re often actually entitled to SMC (r) (2) for that short period before we kick over assuming the proper, multiple causes are service connected (of course). Sadly, since VA doesn’t keep its finger on your pulse, you need to file for these deficits even though the law says VA is supposed to “infer” it. If they can’t see you, they dang sure can’t infer you. Best to file a claim for this just so you’re covered as soon as you see it coming. Doing a verbal “informal” claim on VA’s Dial-a-Prayer/Prize Redemption Line (800 827-1000) is not advised. Seems sometimes they “disremember” that you called. So, without further ado, let’s learn about SMC. I’m warning you ahead of time that this is probably the most confusing system in the VA’s repertoire. One of the highest SMC awards (T) is alphabetically after the second-lowest rating (S) above (K). Go figure.

In the course of this article, you will see the SMC rates expressed as lower case and upper case letters. Ignore that. It takes three strokes to parenthesize (s) versus S. I got lazy while doing this so you’ll see them expressed both ways. Six of one and half a dozen of another. You’ll also learn how to file for two A&A awards under SMC L because VA lets you pyramid your SMC. Interesting? You bet. Read on.
So… Carla. Think of your husband as Mr. Potato Head® for an example. Yeah, I know. In the new, woke world, Mr. P’s getting a lot of negative press. Let’s imagine him as a Veteran starting out complete. Now let’s start removing eyes, arms, legs, breasts and butts and see what happens. He has lost an eye so he gets SMC K number one. Ka-ching–$118.33/month (2022 rates). But, your VSO representative is very, very wrong on the number of SMC Ks you can receive. In the immortal words of Gomer Pyle, Surprise, surprise , surprise, huh? The reason is simple. They don’t teach SMC to VSOs. I can’t tell you why.
 So now, you move forward and say Romeo Tango (Roger That or R/T). Loss of, or loss of use of, a creative organ (we’ll forego illustrating this on Mr. Potato Head™ in order for him to keep his dignity)–Ka-ching. SMC (K)– $118.33 more dollars a month. Each and every condition listed in 38 CFR §3.350 (a) Special Monthly Compensation is a stand alone item worth the $118.33. This set dollar amount is added to your current compensation check for your X% rating disability. §3.350(a) offers eight (8) different losses or losses of use to qualify for SMC K.
So now, you move forward and say Romeo Tango (Roger That or R/T). Loss of, or loss of use of, a creative organ (we’ll forego illustrating this on Mr. Potato Head™ in order for him to keep his dignity)–Ka-ching. SMC (K)– $118.33 more dollars a month. Each and every condition listed in 38 CFR §3.350 (a) Special Monthly Compensation is a stand alone item worth the $118.33. This set dollar amount is added to your current compensation check for your X% rating disability. §3.350(a) offers eight (8) different losses or losses of use to qualify for SMC K.
Obviously, this largesse hits a trip wire eventually. If you are 100% service connected for Hepatitis C and you have some of these items, they are stand alone (K) ratings that qualify. If, and when, the aggregate total of these injuries meets or exceeds what you would be entitled to under SMC L, the gravy trains stops. There is no limit to K awards-other than that you can really only have six if you are at 100% schedular or TDIU and three if you’re at SMC S. The reason is the stricture buried in §3.350(a). If you’re at 100% for $ compensation purposes, the addition of more than six SMC Ks would take you over what is paid for SMC L.
 As I mentioned above, three Ks is the limit if you are at 100% or any SMC rating up to N. But until you attain the 100% (or TDIU), the sky’s the limit as long as you don’t exceed SMC L. One can also see she/he, they, them, theirs would need to have a complete, and boy howdy do I mean a complete Chelsey Manning makeover to get all eight of them. Nobody’s tried to lasso that one yet. Which is not to say it can’t happen. It already did and has since been rescinded. Could be a future President will change it back.
As I mentioned above, three Ks is the limit if you are at 100% or any SMC rating up to N. But until you attain the 100% (or TDIU), the sky’s the limit as long as you don’t exceed SMC L. One can also see she/he, they, them, theirs would need to have a complete, and boy howdy do I mean a complete Chelsey Manning makeover to get all eight of them. Nobody’s tried to lasso that one yet. Which is not to say it can’t happen. It already did and has since been rescinded. Could be a future President will change it back.
SMC, in the words of Robert Chisholm, of Veterans Law firm Chisholm, Chisholm and Kilpatrick, is the art of the possible. It’s so nouveau and the case law is so sparse, it’s a specialized field. VA attempts to suppress knowledge of its very existence. When that fails, VA grants it to sweep it under the carpet. A VA Coach’s Prime Directive is to quash this in its infancy if at all possible. If that fails and you win at the BVA, they welcome you with open arms into the Zeros for Heroes Club and you begin all over again.
Here’s the criteria for (K)
Extremely unfavorable complete ankylosis of the knee, or complete ankylosis of two major joints of an extremity, or shortening of the lower extremity of 3 1/2 inches or more, will constitute loss of use of the hand or foot involved.
Complete paralysis of the external popliteal nerve (common peroneal) and consequent foot drop, accompanied by characteristic organic changes including trophic and circulatory disturbances and other concomitants confirmatory of complete paralysis of this nerve, will be taken as loss of use of the foot.
Which is not to say you cannot win using §3.809. Read Jensen vs. Shulkin to understand it.
The next higher stand alone SMC is SMC (s). Congress is to blame for the SMC alphabet choices. SMC S is a lower value SMC than SMC L-P. To be sure, you may collect the three SMC (k) ratings above as well as SMC (s). By law, your SMC Ks and SMC S cannot exceed the next higher rating of SMC L. SMC S is sometimes called the housebound rating. If you are confined to your home because of medical conditions that keep you home, and your doctor will sign something that says so in no uncertain terms, then you will qualify as “substantially” housebound under §3.350(i)(2) with just a 100% or a TDIU rating.
The most common way Veterans qualify for S is to have a 100% schedular rating or TDIU for a singular disability and a separate, additional 60% or more in combined ratings (using convoluted VA math) unrelated to the initial 100%/TDIU qualifier. Those are the general parameters. VA strictly enforces the singular disability clause. However, one disease process such as Diabetes Mellitus Type II also includes secondaries like peripheral neuropathy and would be considered one disease process. Ditto Parkinson’s disease or IHD with hypertension etc. Now, when SMC S was instituted in 1945-ish, it was reserved for Vets who had served in a time of war only. You didn’t have to be an Eleven Bravo or in a combat theatre but just have served and be in possession of a National Defense Service Medal (NDSM). It’s open to all, now.
Other Veterans Help sites confuse SMC S as somehow being a “lower” form of aid and attendance. It isn’t. VA merely uses the same form- the 21-2680- to determine whether you need housebound benefits or aid and attendance. The form asks certain questions. Depending on how you answer them will determine your eligibility to SMC S or L. If you can’t remember to take your medications due to your condition, or you can’t prepare meals because of your condition, you need a&a. Here’s the form they use.
Now, I get asked this by every single Vet who finds out about this “secret” rating the VSOs never tell you about. “So, dude, I get the 100% check for $3,517.54 a month (2022) and I get the SMC S rate on top of that, right?” Negatory, fellers. VA is on a reduced bonus diet these days. They don’t hand out money like Mardi Gras beads on Fat Tuesday. Think of it like being promoted from PFC to Corporal. In this case, you get a $345 raise per month up from what you were getting with the 100% comp. Think of SMC S as hostile fire pay or a flight pay add on. VA Raters used to tell everyone we Vets call this our ‘Corvette payment’. Yeah, right. $350/month won’t cover a Kia payment.
And here, we enter a footnote -a very important one. Read the following decision on SMC S and what the VA Secretary says about it. The consensus precedent opinion in Howell v. Nicholson says SMC (s) is not based on a medical consideration but a work consideration. I no longer agree with others on this. My take on Howell is read the whole decision and it simply says if you are incapable of leaving the house to earn an income, you are entitled to SMC at the (s) rate based on being truly housebound. The VA likes to say if you can leave the house to attend a c&p exam then you ain’t very housebound. That’s the wrong legal standard of review.
https://asknod.wordpress.com/2014/08/25/cavc-howell-v-nicholson-what-smc-s-really-says/
The regulation(§3.350(i) specifies that you must be either ratable at a combination of 60% worth of separate and distinct disabilities (or more) above a TDIU (or a 100% schedular rating) or with TDIU alone and with extraordinary disability conditions to be eligible. If you have one disease or injury rated at 100% and you are undebatably housebound in all but name only, they may grant. A letter from a doctor would be great help stating as much. Download the 21-2680 form and have your doctor fill it out and then you submit it with a 526 claim form asking for SMC S. Do not let the doctor submit it. SMC S is an extra $397.58 above the normal 100% rating of $3517.84 (with spouse) for a whopping $3915.42/month (2022). A codicil to this is that each and every illness/injury has to be separate and distinct from your 100% (or TDIU item) to qualify. If you have peripheral neuropathy secondary to DM2, those are injuries/illnesses that are distinct and separate but still can be used in combination to qualify for aid and attendance as part and parcel of a single disease process.
Shell fragment wounds to several parts of your body (muscle groups) are all related to one injury or event and are not distinct and separate. VA will get down and dirty on this. Expect a lot of mistakes on what constitutes a “separate and distinct illness above and beyond the primary rating for the TDIU/100%”. They all have to be service connected, too. A complete, different illness separate from the rated one (like cirrhosis (DC 7312)), secondary to the Hepatitis, involves a different element (the liver’s deterioration). Much debate occurs on this and raters make much mistakes after smoking too much M 21. That’s why I write about this.
And before we continue the alphabet disability parade, there are certain times you get a “bye” on a given SMC requirement and advance even higher. Remember, SMC allows you to pyramid certain entitlements. Cool beans, huh?
The next big step up the ladder is the aforementioned SMC L. The requirements of L will invariably carry over some of the (k) ratings because this is an incremental potato head game. L does not hinge on percentages, per se. You need one index disease generally rated as 100% total but the definition of blindness can be argued. Now, I get in arguments with raters at HLR hearings and they point to M 21-1 IV.ii 2.H.8.b. That reference says you have to be rated at 100%. Absent is any mention of TDIU. That’s pure hooey. I’ve gotten Vets SMC L for a&a based on a 50% rating for PTSD. The trick is simple. You have to have “a factual need” under §3.351(c)(3)- read as a diagnosis- that you cannot accomplish one of the items on the list in §3.352(a).
If you qualify for L, it’s $ 4331.94/month in 2022$ as a married Vet. The Forest Gump exemption is still there if you lost your buttocks. If you do, you get to throw in that SMC (k) and any others (up to three) for $103.23/month each on top of your L. That’s not the end of (k)s because you can add them to M and N, too. Oh, and you can keep the (K) for the loss of use of your creative organ too. The fact is, you can keep three of your SMC (k) ratings with an L rating as long as the combination doesn’t exceed what is paid for SMC M. As I mentioned before, it would be pyramiding to collect more than M if you were only rated at L.
SMC L is paid based on any of these:
Need for aid and attendance— The criteria for determining that a veteran is so helpless as to be in need of regular aid and attendance are contained in § 3.352(a). But the regulation saying you require a diagnosis to get it is listed under §3.351(c)(3).
Permanently bedridden–The criteria for rating are contained in § 3.352(a). Where possible, determinations should be on the basis of permanently bedridden rather than for need of aid and attendance (except where 38 U.S.C. 1114(r) is involved) to avoid reduction during hospitalization where aid and attendance is provided in kind. But if you go for bedridden, it wipes out any chances of ever getting two aid and attendance ratings to get to SMC R. I strongly suggest you always fight for a&a.
The loss of, or loss of use of an extremity (hand, foot) is based on the SMC(K) rule (a)(2). This generally is an amputation or impairment closest to the first joint the extremity is attached to. The half steps are for amputation or loss closer to the trunk of the body such as above the knee or elbow. SMC P is a laundry list of odds and ends combined to instruct on all the possible combinations and the proper SMC rating for each. A lot of times the combination of disabilities doesn’t fit a (P) but VA errs on the side of a lower rating.
SMC L pays $4331.91/month with spouse, so this works out to $814.84 more per month than a simple 100% rating. The amount of SMC Ks added to the SMC L cannot exceed what is paid in SMC M-the next higher rate- unless it is described in SMC P. Generally, someone who qualifies for SMC S eventually deteriorates over time and moves up the SMCs to L or M.
Now, if you qualify for L as a stand alone rating based on one disability rated at 100% schedular, and you also had Hepatitis C for 100%, you would automatically advance to SMC (M) See §3.350(f)(4). VA, however calls this SMC “P” because the regulations above are in the P section §3.350(f). If you have a 50% or greater rating on an a disease/injury [regardless of whether the individual diseases, or injuries are of different etiology] and qualify for (L) as a stand alone, then you could theoretically advance with an additional bump to (L½). There is much discussion on this “bump” business. VA raters say the M 21 forbids both bumps. There is currently a case going up to the Fed. Circus on this subject which may settle the question forevermore. (They won. See Barry v. McDonough). I had hoped to defeat that some day because §3.350(f)(3) is wonderfully ambiguous as to whether you can award multiple half-step bumps. If you have a separate and distinct, stand alone 100% schedular rating with award of SMC L, you get a bump from L to M. But you could file for a separate SMC L for A&A for that too. If you had SMC M for LOU of the upper extremities and a 100%, you’d bump from SMC M to N. Under the same theory, you can have a 50% or more rating (or combinations adding up to 50%) and get the 1/2 step bump by VA’s current regulation. Remember its either conjunctively (and)- or disjunctively (or) phrased to understand it. If neither are there for clarification, the regulation or statute that grants the greater benefit is for application. Well, yeah unless you look at it myopically as VA does who tries to minimize the grant. It’s an interesting codicil and one very few raters, let alone BVA judges are even aware of. I’ve found several BVA decisions on this where both bumps- (§3.350(f)(3) and (4))- were awarded.
Here’s an interesting example of bumps. If you had LOU (loss of use) of the upper extremities, You’d be awarded SMC M. If you had another 100% schedular disability for IHD or Parkinson’s, you’d bump up to N. Now that the VA will allow the half-step bump up to N 1/2 as well, and you had a SMC K for LOU of a creative organ, then you’ll get the big bump up to SMC O. Think of it like the kids’ game of Chutes and Ladders.
Obviously, the big banana is to go after two SMC Ls for aid and attendance to reach the higher tier of SMC R1. Most of you will never qualify due to your extremities still being in working order by VA’s estimation. This helps get you around that inequity. I will list these here for your education/edification but the discussion of R1 below is still pertinent.
https://www.va.gov/vetapp21/Files12/A21019424.txt
https://www.va.gov/vetapp18/files8/18126101.txt
https://www.va.gov/vetapp97/files1/9703147.txt
https://www.va.gov/vetapp04/files/0404466.txt
https://www.va.gov/vetapp15/files6/1552412.txt
https://www.va.gov/vetapp18/files8/18125531.txt
https://www.va.gov/vetapp18/files3/1814284.txt
https://www.va.gov/vetapp19/files3/19118790.txt
https://www.va.gov/vetapp19/files4/19125607.txt
https://www.va.gov/vetapp19/files11/a19002711.txt
https://www.va.gov/vetapp21/files2/a21003790.txt
https://www.va.gov/vetapp22/Files6/A22011675.txt
Sometimes I cringe at the thought of publishing these tricks for fear that VA will just change the regs to forbid it. I guess we really don’t have to worry because it isn’t like hordes of VSO service officers are likely to start filing their clients for SMC. Remember, they’ll argue you breathless that this SMC crap is just a fig newton of your imagination and doesn’t even exist.
The next step is SMC (M). Mr. Potato Head™ is gradually losing his ability to ambulate and see if you use the standard approach. He is now wheelchair bound unless he’s very adroit with a bunch of prostheses. Or, if he has a SMC L for a&a and another 100% for IHD or Parkinson’s, he gets the §3.350(f)(4) bump up to M. Or, if he has SMC L for being blind, they bump him up to M if he needs A&A. Always remember this SMC game is like Chutes and Ladders. Here’s the next set of required missing parts if you go strictly by the way the regulation is written on losses of parts and pieces.

5. Blindness in both eyes leaving the veteran so helpless as to be in need of regular aid and attendance. ( You Vets may probably be using this eventually if it’s SC).
Natural elbow or knee action. In determining whether there is natural elbow or knee action with prosthesis in place, consideration will be based on whether use of the proper prosthetic appliance requires natural use of the joint, or whether necessary motion is otherwise controlled, so that the muscles affecting joint motion, if not already atrophied, will become so. If there is no movement in the joint, as in ankylosis or complete paralysis, use of prosthesis is not to be expected, and the determination will be as though there were one in place.
Eyes, bilateral. With visual acuity 5/200 or less or the vision field reduced to 5 degree concentric contraction in both eyes, entitlement on account of need for regular aid and attendance will be determined on the facts in the individual case. In DickandJanespeak, this means you need to get an extraschedular rating for a&a first to get to the point where you can ask to be awarded the bump up to SMC M from L. It isn’t automatic.
SMC M pays $4,761.46/month-an increase up from the $4,546.25/month on (L½). SMC-M½ jumps to $4428.07/month and again requires shorter arms and legs, eyes physically missing, poorly fitting prostheses, etc. Or, being sufficiently blind via a good medical nexus will accomplish this.

SMC N continues the parade of missing pieces. Mr. Potato is now probably blind and immobile due to no feet down belooooow the knees if he relies on the strict reading of it. Actually he’s probably without knees if he’s even seeking SMC N. Or…. think about this. Johnny Vet is blind or nearly so as mentioned above to qualify for SMC M. Using the bump clause, he could get a 100% rating for Major Depressive Disorder (MDD) or even a 100% for IHD or Parkinson’s and then advance from M to N. This is legitimate. I’ve done it for my Vets. Any of the conditions below qualify you for this. Also remember this is the last SMC chance to cash in on the SMC (K) for the lost buttocks/creative organs (or lack thereof). Don’t forget them.
Amputation is a prerequisite except for loss of use of both arms and blindness without light perception in both eyes. If a prosthesis cannot be worn at the present level of amputation but could be applied if there were a reamputation at a higher level, the requirements of this paragraph are not met; instead, consideration will be given to loss of natural elbow or knee action.
SMC (N) pays out at $5390.95/month- a sizable jump from M. I did not include the half steps as they simply add another $200 to the equation and a requirement for a few extra missing pieces or shorter ones. And the last trick in this N gig is if you somehow had a N 1/2 and you drew to a SMC K for loss of use of a creative organ. Bingo! Chutes and ladders again. You get the ladder up from SMC N 1/2 + K to the maximum rate of SMC O.
Rarely are you going to get to N with bumps up from §3.350(f)(3)(4) past going from L to M. At this point, most arrive here totally blind with no light perception. This is not to say you couldn’t have a 100% for IHD and catch the full-step bump up to N and have no physical amputations as I mentioned above. SMC is like an endless river of combinations no one (even VA) could ever conceive of. In some respects, it’s uncharted and sometimes we get into unlitigated pastures never before dreamed of.
I’ve only gotten one Vet to SMC N to be truthful. I’ve always done the chutes and ladders game and advance to Boardwalk and R1 or R2/T. SMC N would be a case of you being amputated down to a torso stump but not needing aid and attendance somehow. Or… if you’re blind, and have another 100% percenter separate and independent from the blindness, you’re in SMC N cotton. It’s really about as superfluous as SMC Q in this day and age. I’m guessing you could liberally count the SMC N Vets in the very low thousands- or even the top tier of the hundreds. These are legitimately Vets who can be bumped to O and thus to SMC R1. Hence the rarity.
When we get to SMC O ($5,237.67) via the standard methods of entitlement , Mr. Potato Head™ would look just that- a potato. However, as you know from the above, this isn’t always the case if you’ve been following some of my shortcuts. Here are the prerequisites to attain (O) via a wheelbarrow of disabilities.

Mr. Potato Head in potato wheel chair.
Intermediate or next higher rate. An intermediate rate authorized by this paragraph shall be established at the arithmetic mean, rounded to the nearest dollar, between the two rates concerned.

Mr. P head on R1
SMC (O) is generally as high as you go unless you have two 100% disabilities distinctly different from one another and one of them is Aid and Attendance at the L rate. A bright line rule when you get into the higher levels of SMC or leapfrog ahead under the §§3.350(f)(3),(4) codicils is to expect to have to meet stringent requirements. I’ve seen how VA treated one Vet in just the last year (2016). He was housebound, has grand mal seizures that put him in the hospital for two weeks at a time. He loses his recent memory and has to “catch up” after each seizure. He can successfully transition from his bed to his wheelchair without falling so VA considers that proof that he has not lost the use of his lower extremities (entitling him to a jump from SMC P (M + K+K) to SMC R1). That took several doctors and employing the correct DBQ on the subject. They somehow disremembered they were not supposed to use the DBQ for Peripheral Neuropathy.
Here’s an interesting rating using SMC O and the addition of another A&A rating under L to get to R1.
https://www.va.gov/vetapp98/files1/9802978.txt
SMC P is what throws everyone. There is no set pay for SMC P so you have to retreat to §3.350(f)(1). Trust VA to try to envision every possible combination of a SMC L or M rating and begin adding on Ks and lengths of limbs capable of strapping prostheses to. Nevertheless, they did it-more or less. Check out all these myriad possibilities and see if you can squeeze into one some day.
(1) Extremities.
(i) Anatomical loss or loss of use of one foot with anatomical loss or loss of use of one leg at a level, or with complications preventing natural knee action with prosthesis in place, shall entitle to the rate between 38 U.S.C. 1114(l) and (m). L ½ $3,977.97 (2015)
(ii) Anatomical loss or loss of use of one foot with anatomical loss of one leg so near the hip as to prevent use of prosthetic appliance shall entitle to the rate under 38 U.S.C. 1114(m). M $4,166.28
(iii) Anatomical loss or loss of use of one foot with anatomical loss or loss of use of one arm at a level, or with complications, preventing natural elbow action with prosthesis in place, shall entitle to the rate between 38 U.S.C. 1114(l) and (m). L ½ $3,977.97
(iv) Anatomical loss or loss of use of one foot with anatomical loss or loss of use of one arm so near the shoulder as to prevent use of a prosthetic appliance shall entitle to the rate under 38 U.S.C. 1114(m). M $4,166.28
(v) Anatomical loss or loss of use of one leg at a level, or with complications, preventing natural knee action with prosthesis in place with anatomical loss of one leg so near the hip as to prevent use of a prosthetic appliance, shall entitle to the rate between 38 U.S.C. 1114(m)and (n). M ½ $4,441.36
(vi) Anatomical loss or loss of use of one leg at a level, or with complications, preventing natural knee action with prosthesis in place with anatomical loss or loss of use of one hand, shall entitle to the rate between 38 U.S.C. 1114 (l) and (m). L ½ $3,977.97
(vii) Anatomical loss or loss of use of one leg at a level, or with complications, preventing natural knee action with prosthesis in place with anatomical loss of one arm so near the shoulder as to prevent use of a prosthetic appliance, shall entitle to the rate between 38 U.S.C. 1114(m) and (n). M ½ $4,441.36
(viii) Anatomical loss of one leg so near the hip as to prevent use of a prosthetic appliance with anatomical loss or loss of use of one hand shall entitle to the rate under 38 U.S.C. 1114(m). M $4,166.28
(ix) Anatomical loss of one leg so near the hip as to prevent use of a prosthetic appliance with anatomical loss or loss of use of one arm at a level, or with complications, preventing natural elbow action with prosthesis in place, shall entitle to the rate between 38 U.S.C. 1114 (m) and (n). M ½ $4,441.36
(x) Anatomical loss or loss of use of one hand with anatomical loss or loss of use of one arm at a level, or with complications, preventing natural elbow action with prosthesis in place, shall entitle to the rate between 38 U.S.C. 1114 (m) and (n). M ½ $4,441.36
(xi) Anatomical loss or loss of use of one hand with anatomical loss of one arm so near the shoulder as to prevent use of a prosthetic appliance shall entitle to the rate under 38 U.S.C. 1114(n). N $4,717.07
(xii) Anatomical loss or loss of use of one arm at a level, or with complications, preventing natural elbow action with prosthesis in place with anatomical loss of one arm so near the shoulder as to prevent use of a prosthetic appliance, shall entitle to the rate between 38 U.S.C. 1114(n) and (o). N ½ $4,984.98
(2) Eyes, bilateral, and blindness in connection with deafness and/or loss or loss of use of a hand or foot.
(i) Blindness of one eye with 5/200 visual acuity or less and blindness of the other eye having only light perception will entitle to the rate between 38 U.S.C. 1114 (l) and (m). L½ $3,977.97
(ii) Blindness of one eye with 5/200 visual acuity or less and anatomical loss of, or blindness having no light perception in the other eye, will entitle to a rate equal to 38 U.S.C. 1114(m). M $4,166.28
(iii) Blindness of one eye having only light perception and anatomical loss of, or blindness having no light perception in the other eye, will entitle to a rate between 38 U.S.C. 1114 (m) and (n). M½ $4,441.36
(iv) Blindness in both eyes with visual acuity of 5/200 or less, or blindness in both eyes rated under subparagraph (2) (i) or (ii) of this paragraph, when accompanied by service-connected total deafness in one ear, will afford entitlement to the next higher intermediate rate of if the veteran is already entitled to an intermediate rate, to the next higher statutory rate under 38 U.S.C. 1114, but in no event higher than the rate for (o).$5,253.39
(v) Blindness in both eyes having only light perception or less, or rated under subparagraph (2)(iii) of this paragraph, when accompanied by bilateral deafness (and the hearing impairment in either one or both ears is service-connected) rated at 10 or 20 percent disabling, will afford entitlement to the next higher intermediate rate, or if the veteran is already entitled to an intermediate rate, to the next higher statutory rate under 38 U.S.C. 1114, but in no event higher than the rate for (o).$5,253.39
(vi) Blindness in both eyes rated under 38 U.S.C. 1114 (l), (m) or (n), or rated under subparagraphs (2)(i), (ii) or (iii) of this paragraph, when accompanied by bilaterial deafness rated at no less than 30 percent, and the hearing impairment in one or both ears is service-connected, will afford entitlement to the next higher statutory rate under 38 U.S.C. 1114, or if the veteran is already entitled to an intermediate rate, to the next higher intermediate rate, but in no event higher than the rate for (o).$5,253.39 (Authority: 38 U.S.C. 1114(p))
(vii) Blindness in both eyes rated under 38 U.S.C. 1114 (l), (m), or (n), or under the intermediate or next higher rate provisions of this subparagraph, when accompanied by:
(A) Service-connected loss or loss of use of one hand, will afford entitlement to the next higher statutory rate under 38 U.S.C. 1114 or, if the veteran is already entitled to an intermediate rate, to the next higher intermediate rate, but in no event higher than the rate for (o); or
(B) Service-connected loss or loss of use of one foot which by itself or in combination with another compensable disability would be ratable at 50 percent or more, will afford entitlement to the next higher statutory rate under 38 U.S.C. 1114 or, if the veteran is already entitled to an intermediate rate, to the next higher intermediate rate, but in no event higher than the rate for (o); or
(C) Service-connected loss or loss of use of one foot which is ratable at less than 50 percent and which is the only compensable disability other than bilateral blindness, will afford entitlement to the next higher intermediate rate or, if the veteran is already entitled to an intermediate rate, to the next higher statutory rate under 38 U.S.C. 1114, but in no event higher than the rate for (o).$5,253.39
So, if you still find your self lost in SMC P’s possible manifestations, you now know how all those chuckleheads at the VARO feel when they get to figure it out. The general rule is you’ll be lowballed -especially on the effective date. Remember, in SMC world, it’s not the day you filed for it to get the entitlement. Whoa, Nelly. It’s the day you can prove you’re entitled. You don’t even need to have the proof in the VA’s constructive possession. If your medrecs show you were permanently bedridden in 2008, then by golly that’s your date of entitlement to SMC L for that particular SMC facet.
The easiest way to get to R1 is the most obvious- §3.350(e)(1)(ii). You start at SMC L. If you are entitled to Aid and attendance, you are awarded SMC L #1. If you should also lose the use of both your lower extremities, or an upper and a lower extremity, you get another SMC L- #2. Two SMC Ls or any combination of of two Ls, Ms, or Ns gives you a bump to SMC O automatically. SMC N ½ with a K will advance you to O too. But-here comes the legal pyramiding- if you have two of any of the rates between L and N, with no condition being counted twice, and one of the ratings is for Aid and Attendance, you advance to SMC R 1 automatically. No VSO has a clue how to play SMC Chutes and ladders. It requires a lot of study to understand the myriad ways you can do this. It’s an art form building them and requires getting rated for the prerequisites, often in a carefully specified order) and then springing the trap on them before VA realizes they just handed you the Claymore to ambush them with.
I advise getting the A&A first. As previously mentioned, you can also get two A&A awards for separate disabilities that require A&A. This, too, will advance you to R1. You’ll actually find in practice that if you file for loss of use of extremities, they’ll default to SMC L a&a in hopes of fencing you out of it. Cool beans. You then just get an IMO saying your legs are hors d’combat and get R1 that much sooner.
R¹ ($8499) and R² ($9721) (married 2022) are ratings for more extensive Aid and Attendance and are considered an extension of SMC (O). If you know how, you can attain this and still be “alive”-i.e., not a baked Mr. Potato Head™. It seems sad when viewed in this context but a Vet has to almost be nigh on to Helen Keller in the VA disability world to get to N. Lt. Dan of Forest Gump fame would only qualify for M for his two amputations above the knee absent IHD or PTSD at 100% or full-blown Parkinson’s. My Uncle Jay with one foot destroyed (and amputated above the ankle) by a through-and-through GSW had 40% and two Ks, the other for loss of use of a creative organ before they caved in and gave him 100% P&T for PTSD. One thing is for certain in the Potato game- know your regulation and which SMC you may qualify for because VA is not in the habit of researching it for you and including it in the next paycheck-most especially not the higher SMCs. Considering most VSOs have never heard of R1, it behooves you to be acquainted with it if you’re using one to file for it. Well, that or call me to do it for you.
The easiest way to make the jump to R 2 is to be seriously R 1 first. The added need for a higher level of A&A (R 2) is most easily accomplished if you-the caregiver or spouse-are officially “trained” by your supervising neurologist or Doctor to provide physical therapy and things like changing the undergarments due to incontinence. “Cleanup on Aisle 2” will suddenly take on a new meaning. A candidate for R 2 must be so helpless that, without the help, he would have to be institutionalized in a hospital or nursing home. Personally, there are a large number of R 1s out there in VA Land who qualify for R 2 but lack the intricate knowledge I offer here free to argue it successfully. Rest assured that no VA examiner or rater can figure this out so they deny to avoid exposing their ignorance. VA has a “SMC Computer” where you put in the ratings and it spits out the magic SMC(s) entitlement. The problem is the input. I’ve only had two R 1s granted at the local level (Waco and Little Rock). A DRO in Ft. Hamilton, Montana told me they always send these to DC unless someone is bedridden and dying…and the conditions are separate and distinguishable.(Breniser v. Shinseki, 2011)

Mr. Potato Head at SMC R2
Higher Special Monthly Compensation is a benefit America accords its most damaged Vets. As you can see, Congress was might picky about how short an arm or leg had to be to get another $250.00 for it. VA sure wouldn’t want us gold diggers trying to game the system. I have visions of Spanish Inquisition torture devices to stretch a Vet’s arm or leg to get him on the wrong side of an SMC requirement. I’m sorry. I’m jaded. They have hurt me so frequently I’m damaged goods and no longer trust them. But… I have two separate and distinct 100% disabilities and am looking forward to my wheelchair license and a bump to SMC L. Hell, if Winky quits working, I may get a K thrown in too which would take me up to P-something.

Early versions of VA Range of Motion Improvement devices circa 1945
A a matter for dissection, let’s look at my collection of disabilities. The moment I lose the use of my lower extremities due to my airplane crash, I’ll advance from SMC S to L for aid and attendance of another. Please recall that you do not take the SMC S and add it to SMC L. No way, GI. You leave it behind and get promoted to L. Having arrived, I will then exercise my extra rating for 100% for my Porphyria or my under §4.115a (dialysis) or my 100% for Hepatitis C. This bumps me up automatically to SMC M. If winky quits working, I go SMC P (M+K). No VSO will tell you this. Most probably wouldn’t know it could be done. That would be the difference between $4331 a month versus $5075 (married) in 2022 $. Spooky, huh?
The M 21 says you cannot use both a 100% bump and a 50% bump even if you qualify for each. This changed in Barry v. McDonough on May 16, 2024 and multiple (f)(3) half-step bumps can now be done. The regulation (§3.350(f)(3) and (4) are the pertinent authority Not (f)(4) but (f)(3). (f)(4) is strictly interpreted to allow one bump only. Barry Vs. McDonough.
I can see the look of astonishment dawning on some of your faces when you think back to that VSO Rep from DAV saying there simply was no more dough after you got to 100% and told you to go home and quit being greedy. Shoooo doggies. 100% is $3517 (married in 2022) and SMC S is $3915 (married). You’ll begin to see why this looks like the Mekong Delta with all the possible combinations and switchbacks. SMC O purposefully allows the double counting (pyramiding of ratings) to get to R1 or R2. It’s the only instance of the violation of 38 CFR §4.14 in the entire CFR that VA sanctions. From the number of comments I get on this blog, I apologize if I do not answer all of them. SMC is the most misunderstood system of entitlement in the VA system of compensation. It took me four years to say I have it somewhat memorized-both the regs and what they say. I pretty much have all the cites to Court precedence memorized as well. That really helps when you don’t have to keep looking down to recite stuff at a BVA hearing. You can look the Judge right in the eye and pin him like a deer in the headlights. I always catch the Judge digging into the 38 CFR Part 3 or 4 to check up on me during the hearing or writing/typing fast and furiously. Cool beans, huh? You need as much ammo as you can hump, folks. That’s it in a nutshell.
Always remember. Only the rater or a trier of fact (VLJ) can grant you R1. see M21-1, IV.ii.2.H.1.b. It says the clinician cannot diagnose loss of use of extremities even though I see it on a lot of DBQs. You’re wasting your time going out and getting your doctor to say your legs are toast. But, once they deny you, you can go out and get the magic DBQ saying you have LOU. https://www.vba.va.gov/pubs/forms/VBA-21-0960C-5-ARE.pdf
Look at page 8 in Section X below. Right there it asks the clinician to determine that you have loss of use of extremities that would qualify you for loss of use of upper or lower extremities. As I like to point out to Judges, M21-1, IV.ii.2.H.1.b. doesn’t say you cannot rebut VA’s finding with your own diagnosis. I use the Caluza/Hickson/Shedden and its progeny to support the right of any Veteran to supply the three ingredients needed to prevail. VARO examiners have some unknown “higher level” legal standard of review on loss of use but cannot provide it at a hearing or HLR conference call. You almost always have to get the VLJ to grant because no one wants that on their resume when they’re going for the Christmas bonus or a big jump up to GS 13, step 5.
P.S. The dollar rates I listed for all these SMC Rates constantly change due to COLA rates increasing annually. I used to circle back and correct them to the current year but it’s too time-consuming now that I am accredited. Most of the rates advertised were for 2022. Obviously, SMC K is at $118.33 in 2022 now. Ignore that. The financial reward is immaterial to the discussion. To check the current rates, use my widget at the top of the blog. (VA Comp)
I don’t expect Joe Average Veteran to soak up this knowledge in one reading…or ten for that matter. SMC is antithetical to rational thinking when doing VA claims. Personally, I’d suggest any who try to do this get an attorney or agent who is well-versed in it. VA is vicious in this arena. They lie and misquote regulations. They add requirements that are not there. They ignore pathways to two a&a ratings and declare there’s no such thing. I tell my clients SMC is the art of the possible but most often requires appeal to the BVA to find a receptive ear and a keen legal mind-i.e., a lawyer/VLJ rather than a GS 13 VA examiner with a hardon for anyone asking for High SMC.
And that’s all I’m going to say about that.
Win or Die.

P.S. I wrote this in 2013 and have added, expanded and rewritten parts as the law changes. I became accredited in 2016 and learned even more about SMC from the owner of CCK. This represents the best knowledge I can provide to you, my Veteran brothers. I give it freely because no Veteran should have to pay to play this game. No pay walls. No inner sanctums. Getting the highest rating you are entitled to, especially the higher SMCs, requires a lot of specialized knowledge. I like to point to the analogy that just because you know how to drive doesn’t ensure you are Indianapolis 500 driver material. If this helps even one Veteran get to R1, R2 or T then it was well worth my time invested in it. Best of luck to you all.
PPS. I promise to share my SMC T adventures here. It’s actually easier than getting R1. Time and my heart are my enemies. On second thought, revealing all my SMC T tricks here would just let VA know them too.
PPPS. And, lo and behold, the Federal Circus (CAFC) agreed, in Barry v McDonough on May 16, 2024 that a Veteran can have more than one half-step bump under §3.350(f)(3). In fact, they said there was no limit to how many half-step bumps one could be awarded.
so, how about this one.
This just in. After reading their cards and weeping, VASEC has just acknowledged they are holding what appears to be a compromised or losing hand. Oddly enough, it only took them 5 years to ascertain this (2008). I guess someone sat down and read the file instead of continuing to blindly fight on.
From: Purcell, Emily [mailto:Emily.Purcell@va.gov]
Sent: Wednesday, February 27, 2013 9:13 AM
To: Robert P. Walsh
Subject: Nodster CAVC #12-XXXX
Hi Mr. Walsh,
The Secretary can agree to remand the issue of the Board’s denial of entitlement to an effective date earlier than February 23, 2007, for the grant of service connection for Hepatitis C. The remand would direct the Board to provide adequate reasons or bases for how the January 1995 SOC clearly conveyed to Appellant that the decision on that claim was final. In order to enter into a JMR, however, we would need Appellant to abandon the tinnitus claim and arguments pertaining to CUE. Please let me know at your earliest convenience whether this is something that Appellant is interested in pursuing.
Thanks,
Emily
Emily C. Purcell
Appellate Attorney
U.S. Department of Veterans Affairs Office of the General Counsel (027K)
810 Vermin Avenue, N.W.
Washington, D.C. 20420
In an effort to appear grandiose, they have condescended to allow one of the following:
1) a remand back to the BVA for a restatement of how the 1995 SOC was clearly a denial. This will attempt to show that the following should have amply warned me that my claim had been denied…
Scenario #2 will be a Joint Motion for Remand (JMR) which will hash out their surrender and the terms of my 1994 rating. As you can see, VASEC has already started putting in preconditions that require me to drop my tinnitus appeal and to withdraw my CUE claim.
Law Bob, being a gambler like me, stated the obvious. “The bid is now 3 no trump”. VA has suddenly realized their legal arguments are akin to screen doors in submarines. However, since they are so munificent, they are willing to accept my apology and hand out old Halloween candy if I throw in two claims.
I would ask Bob to think back on General Anthony McAuliffe’s response when he was asked by the Germans to surrender in 1944 at Bastogne.
So, in sum, since I am in possession of a full house, why should I acquiesce to a remand all the way back down to Fort Fumble in Seattle and get the traditional Fenderson 0% fight for 5 years? Either VASEC offers the 60% from 1994 or we go to trial and let VASEC explain in his best post hoc rationale that VAOP OGC PREC 9-97 doesn’t mean exactly what it says it means or that the 1995 Statement of the Case was a typo and I should have understood that at the time.
Stay tuned to the next exciting adventure. Same CAVC time. Same CAVC channel. News and film at 6.
After years of zooming by 38 CFR §3.303(b) like an anonymous building alongside the freeway at 65 mph and seeing it quoted often in denials of HCV cases, I was rudely awakened to the following. Apparently a lot of us pro se idiots were misinterpreting it to encompass diseases as well as injuries like degenerative disc disease. No way, Jose. Mr. James E. Walker and I just got an education in what the regulation says, and most importantly, what it doesn’t say. Oddly enough, the VASEC apparently has been lost in the same fog and finally stumbled out of it with an interesting legal epiphany.
38 CFR §3.303 has been around in one form or another since 1947 so it isn’t some new mission creep, post hoc rationalization trotted out for the first time in a dastardly attempt to create new law or precedence. It pretty much means what it says. It encompasses in section (a) much what 38 USC 1154(a) does in how the rating shall be based with due respect on the what you and your organization were up to during your service. If your platoon was effectively wiped out and you survived, it could be said that you deserve the combat accommodation in §1154(b) as well.
They throw in the benefit of the doubt at the bottom just to make it look fair.
In the red above, please note that it mentions both disease and injury. Now parse §3.303(b)…
Wow. Big uh-oh. No longer can you point to a back injury in service and a current, ongoing, chronic injury and say it’s the same one by basing your argument on §303(b). You will have to rely on your SMRs and the word “chronic” mentioned there. Any nexus letter will also have to discuss quite a bit of medical science and why the doctor came to the conclusions he did. 38 CFR §3.303(a) will now be the default setting for all “injuries”.
VA has probably under-enforced this for years, or, on the other hand erred in favor of the Vet with a generous interpretation. That will all be erased by a quick revamp of the M21-1MR to regurgitate all the prior ones for a redo based on CUE.
Walker is going to be anathema for years until a new defense based on other legal facets can be fashioned out of 38 USC Part 3. Either that or someone is going to have to pull their plug and go upstairs. The CFRs, being an invention of VASEC, merely interpret the Statute. If they become overly broad and are determined to be too restrictive for Vets or overreaching, they’ll be trimmed like the proverbial hedge.
Herein lies the poison pill:
This one sentence will be quoted for a long time.
Here’s the bombshell in footnotes 3 and 4 (pages 13 & 14)…
This is over the top. The Federal Circus has already ruled in the positive in Groves v. Peake and now they are striking it down. Groves was a fine, well reasoned piece of law that adequately accommodated §3.303(b) in the context that a mental disease in service was the same (chronic) after service. As you can see, they stepped on their necktie and are attempting to revamp established precedence. This isn’t over. I can see Mr. Walker’s leagle beagles headed straight to the Supremes for certiorari. Whether they get it or not is going to be intriguing. The rending asunder of years and years of work (and established precedent) cannot be done so arbitrarily or lightly. By reading §3.303(b) as they did for this long, they have inadvertently given their seal of approval to it. In this matter, Walker is now settled law and a new “finding”. The Feds are trying to go back and erase that which came before. Abrogating Groves and a host of other similar ones like Savage, Kent and Barr is going to set Veterans rights back on their heels. A large vein of jurisprudence is predicated on just Savage alone.
The BVA and VAROs can actually have a field day with this and undoubtedly will. Watch how quickly this is inserted into the mix. I know in 1992 during my BVA decision that numerous new precedents like Wilson and Shafrath were ignored for months, if not years, even though promulgated as much as 90 days previous. Don’t be fooled. Walker can’t stand as it is. Too much goes down the tubes with this. The Feds have been granting it for almost a decade. VASEC hasn’t protested once (until now). This smacks of a way to have more denials and thus fund more Human Rights seminars in Costa Rica.
Eventually, the Supremes could rule that VA has been doing it this way for years so why the bitch all of a sudden. Isn’t that the favorite complaint from VASEC when they are caught rearranging the judicial regulations to mean new things? Oddly, the VASEC is on very firm legal ground but indefensible inasmuch as he has never put his foot down and complained. To do so now smells of desperation and a desire to be vindictive. He’s convinced the Feds to go along and they are only obeying the undisputed reading of §3.303(b). Arguments about §3.309 missing from it are specious and cannot rise to the level of it being flawed.
Say what you will but §3.303(b) is one of those tar babies the VASEC forgot to keep track of for the last sixty six years and now wants a do over on. It would appear he has it. Anyone who obtained ratings based on this with less that 10 years under the belt stands a darn good chance of being pulled in and having it removed. For those of you with less than five years, I think we can say Sayonara to any Savage or Barr jurisprudence. Time will tell if this will stand. Earth shattering would be a good synopsis for Vets.
And if you thought the backlog was ginormous before, wait until you see the VA crank up the CUE machine on all these erroneous grants based on Savage v. Gober and its progeny. This may get ugly. What the hey? Now VASEC has another excuse for why 2015 and 125 days is right out.
Thus we award the Alfred (I don’t care about Vets) E. Neuman award to the Federal Circus this month for finally putting their glasses on and actually discerning the difference between 38 CFRs §§ 3.303(a) and (b).
http://caselaw.findlaw.com/us-federal-circuit/1622844.html

What? Me worry about whether it says “diseases”? No way. I see it now so no harm, no foul. Got it? Make it so, Numbah 1.


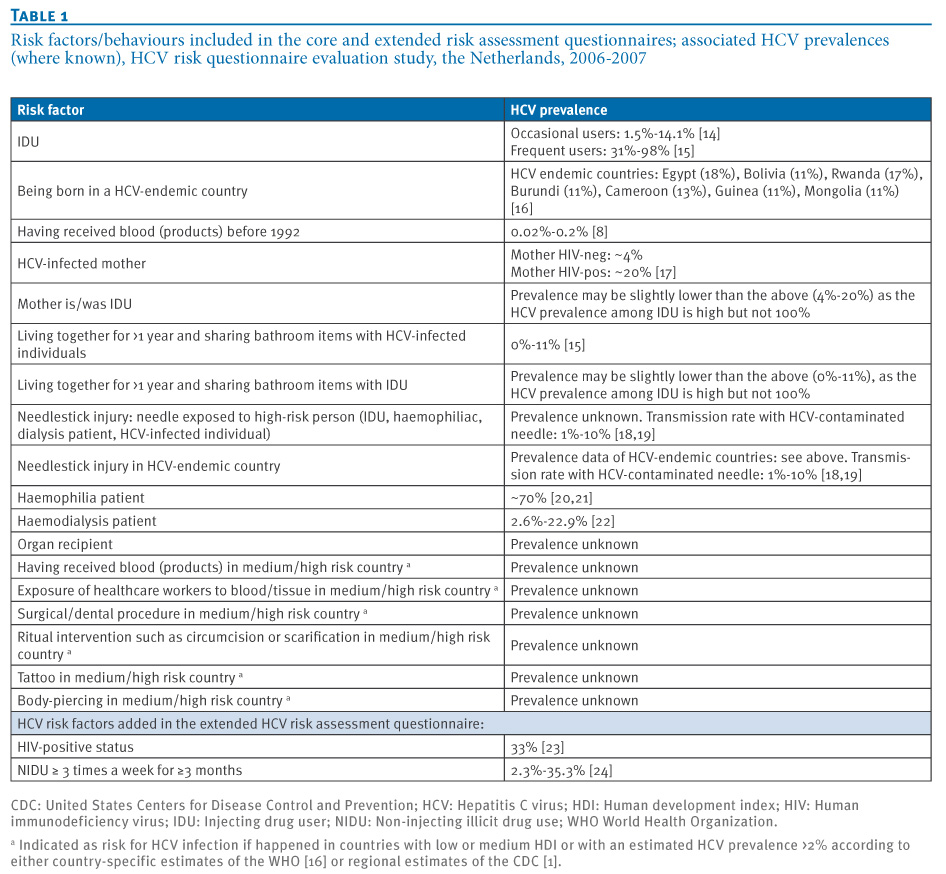{kind=link}