
The DOD began screening applicants for HIV in 1985 and rejected anyone who tested positive. In those days, it is estimated that a person died from AIDS about 10 years after becoming infected with HIV (J. Pepin). Each country has a different demographic profile for the epidemic. As we know, in the U.S., HIV/AIDS was first described in the gay male population and continues to affect the MSM group the most (50%).
One can think about the U. S. military as a country or “transmission category” even if the CDC doesn’t publicly. This country is made up of mainly old non-white men, probably heterosexual (although the VA doesn’t collect that data) and like the vast majority of Americans, have never injected illegal drugs into their veins. Many are also co-infected with HCV.
A few figures from a GAO report about the VHA reveal that there were about 22.2 million living veterans on Sept. 30, 2011 and about 5.2 million veterans received health care from the VHA–or roughly 17 million or 24% if my arithmetic is correct. So about 75% of veterans receive their health care outside of the system.
The VA reports that over 25,000 HIV-infected Veterans received health care in VHA. In 2009,
about 1 of every 250 Veterans in VA health care was living with HIV/AIDS.
If the “1 of every 250” veterans with HIV holds true for veterans being treated outside of the VHA, about 68,000 are infected. Veteran status looks like a HIV risk factor to me.
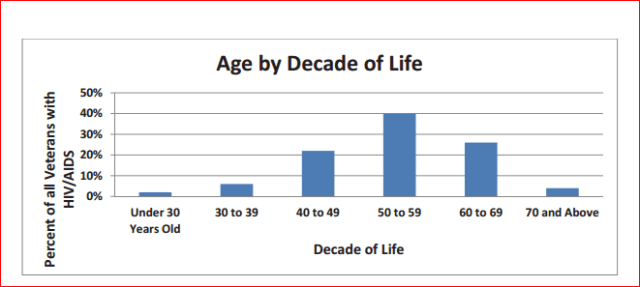
This 2011 VA chart is interesting because it shows that most veterans in VHA care are oldies with a median age of 54 and 30% over 60 years.
HIV Infected Veterans in VHA Care 2011 – Age by Decade of Life
Elderly veterans with HIV
In general, the earlier HAART treatment begins, the longer a person can expect to live so this is a good trend.
This hopeful table is copied from a Harvard article:

In-service tattoos and sexual activity, are certainly important (evidence-based) ways that HIV spread post-1985 although the RO and BVA shoot down claim after claim. The blood supply/blood products got safer in the early 199os we’re told.
Illicit IV drug users spread blood-borne pathogens like HIV and HCV efficiently but so do all invasive medical procedures that aren’t sterile. Just today the news reported about a private dentist in Oklahoma who has surrendered his license after an inspection showed that he had exposed his patients to infections like HIV and HCV. If there was no inspection, there would be no way patients could prove that they were infected in his office, should that be the case. These nightmarish stories are getting common.
The BVA judges get all gleeful if a veteran with HIV proposes a new in-service risk factor at some point in his claim process. “Ah HA!, First he said he got HIV from the jet injectors. Later he said, he said he became infected from combat blood exposure! You loser, go away. And stay away.”
What the heck! Are veterans supposed to have honorary degrees in Epidemiology?


Had our own Colorado case of a dentist who surrendered his sheepskin after alledgedly contaminating over 1,000 patients. Good thing I have a reputable dentist and although extremely tired feeling good on all fronts (and sides) thus far.
Yes, the Colorado dentist made the headlines too. In Oklahoma, the health officials say they don’t have the manpower to inspect all 10,000 dentists.