![]() Before I begin this
Before I begin this diatribe-nay-observation, I have something that needs to be illuminated. I don’t spend much time on my phone. If I did, nothing would get done. Personally, I think that’s what’s happening to the rest of the world these days. On my Gargle™ news feed, I have gradually accumulated about ten questions that just beg to be answered. I’ve never clicked on the items to find out the whyhow. I don’t think there’s enough room in my wallet for all the items either. Read on.
 This conundrum deserves a brewski/wine seltzer and some Snyder™ Pretzel sticks with extra butter at a minimum and then you can return to watching the NFL further demean America by avoiding playing the National Anthem before the game to appease the 1% of our poor conflicted/offended players.
This conundrum deserves a brewski/wine seltzer and some Snyder™ Pretzel sticks with extra butter at a minimum and then you can return to watching the NFL further demean America by avoiding playing the National Anthem before the game to appease the 1% of our poor conflicted/offended players.

The bread clip ‘don’t leave home without it’ admonition
I spotted this one about four years ago. Being inherently lazy and busy to boot, I’ve just never put the world on pause to find out what dire trouble I’ve been in all this time and how that bread doomoflotchie is going to make me a) rich, b) thinner; or c) get back on the WWP™’s Christmas Card list.

The Crayola™ crayon ‘don’t leave home without it’ caution
This requirement came and went far more rapidly than most. I haven’t seen it in years now. Either the good folks at Gargle™ found a way to combine the crayon need with the Bread Clip need or one of the others on this list below may be the reason we no longer need crayons to save our asses. Knowing crayons tend to melt on hot days, I thought immediately of how they might fare in a 98.6° wallet.

The ‘Do this to your phone by Sunday’ warning
This is actually flexible. The admonition could be any other day of the week as long as it’s two or more days hence. That’ll give it a suitable sense of urgency. If you’re mega insecure, you’ll probably fall for all these ploys-even the every day of the week ads on fixing the phone with your handy shish kabob from the kitchen-or is it a toothpick?

The tinfoil trick of wrapping the door knob for when you’re in a hotel
That one always invigorated my attention. Does this have something do with the Corona Virus? Are there coodies on the knob? What if the knob is a lever and not a round knob? What do you do then? Will Saran wrap work or does it have to be tinfoil? Shoo doodle. Making room in the wallet for the bread clip, the crayon and now tin foil? Pretty soon I’m gonna need one of them ‘man purses’ to cart all this crap around.

The ‘Put a water bottle on top of the tire’ warning device
This one may save your life. Well, it sure sounds that way. One thing’s for sure. Pretty soon the folks at the Hampden Inns™ and Motel 6’s across our fruited plains are going to get sick and tired of picking up all your water bottles and recycling them for you. Eventually, they’ll fine you for it if they see you do it. It could be you need to go back and check out the Bread Clip gig and or the crayon/tinfoil tricks to see it you can substitute them in lieu of the water bottle.

‘One teaspoon of this every night before bed and watch the weight fall off”
Well, to begin with, I’m 72 and in all those years I’ve never been personal witness to this phenomenon. I’ve seen a lot of stuff fall off things. Tires fall off cars. Nape and CBU fall off the hard points on a wing. Once a guy lost his camper shell off the back of his pickup truck and it sailed right over the top of my rig. I almost had one of those urinary/fecal moments in my pants to be truthful. I guess that might qualify for weight falling off and it doesn’t require a teaspoon of anything.

‘Here’s how much you need to save to be able to retire by 38’
Personally, I think you should also include some pointers on what kind of business you need to be in to pull down this kind of dough. My guess is it involves buying into the Dave Del Dotto™ patented Cash Flow System or you’re gonna need to move a shit ton of Fentanyl every week with your brand new best friends forever in the Mexican Cartel. I reckon flipping houses is right out by now. Even if you could find a house you could afford to pick up for a song and a dance, you’d still need some serious folding cash. Bidenomics is rapidly pricing you out of this future.

THE BVA/VBA DEBACLE
This is a real bone of contention with me. Not just because I do claims for Veterans but because as long as I’ve been doing it, the siren lure of Drive Thru lanes at the Regional Offices has always been touted as just around the corner. Under Secretary for Benefits (USB) Allison Hickey promised as much to Congress several times. Each promise was premised on the completion of electronic records files in the near future and an infusion up front of some Baksheesh right now to implement it. Alas, each time defeat was snatched from the jaws of success as some unfortunate event intervened and the magic 125-day claim from start to finish was thwarted. Fortunately, the infusion of more shekels was capable of righting the wrong and accomplishing this worthy goal.
So, here we stand, almost ten years later and the 125-day plan still eludes the bean counters. Could it be that they need bread clips or crayons to fix this? I decided to do a dumpster dive in my VBMS feed this morning to see the “average” delay in the claims based solely on my miniscule effect on the system. The average, even when pulled up statistically by several new clients’ submissions in the last 14 days failed to move the needle away from some ugly numbers. I count 21 of my active 40-odd pending new and supplemental claims are well over 125 days-most over 200.

I have a surviving spouse for whom I filed claims as her husband entered hospice. This was back in late 2021. He wasn’t going to make it but there’s no law that says you can’t file for a&a at the end. Sure enough he punched out in March 2022 so there were already four months on the odometer. First thing is they “lost” the claim simply by cancelling it. This was humorous because they’d already received ACE (acceptable clinical evidence) c&p exam opinions back as to whether it was or wasn’t service connected (SC). Fact is they sure didn’t have any problems granting her DIC and burial benefits within 125 days. I reckon that claim-before-death thing was just way more complicated. From the looks of it, I’d say they were praying we’d just disremember it and it would all go away. What the hey? The Vet’s dead. He sure ain’t gonna get to spend it. Right?

I got the claim reestablished after a lot of screaming. However, the new 125-day clock began the day they “found” the old claim and restarted it. You can do the math. The claim was just denied a few weeks ago. It should have registered as about 455 days. But that’s nothing compared to the BVA’s backlog. Even worse, this ‘oops we accidentaly cancelled it’ game isn’t a fluke. I’ve had about 15 of those that required massaging to bring them back to life. Every last one involved a deceased Veteran. Coincidence? You be the judge.

When VA and the Big Six VSOs hornswoggled Congress into the new AMA revision so as to enable lightning -fast adjudications, they used the same old snake oil they’ve been selling for decades. Granted, I guess they didn’t see the Procopio 12-mile Blue Water Navy exception coming- but they did, really. Eugene Haas’ denial (Haas vs. Nicholson) about where the AO ended began this problem way back in 2006. Up to then, if you had a Vietnam Service Medal (VSM), VA pretty much granted service connection for AO crap. Then some bean counter at VA discovered Thailand Veterans were awarded VSMs, too. That began a massive do over and a gazillion CUEs to weed them out. Then they noticed the Squids out in the South China Sea were, too and bingo-that party ended until Procopio was decided. And now we have the PACT Act granting AO to Thailand, Anderson Island and every whistle stop between Saigon and San Diego.

Suddenly, after Haas, being in the “Boots on the Ground Club” became far more exclusive. You needed some pretty hard evidence to prove it. We began resorting to using the old Yellow Shot Books to prove incountry via the APO zip code. I even used a letter a Vet sent to his parents with the “Free” franking stamp in the upper right corner where the stamp goes. Credibility only goes so far at the VA. Merely stating you made the weekly Klong flight from Yankee Station to Da Nang to pick up the mail, Marbs and the brewskis wasn’t good enough. You had to show your MOS was mail carrier.

This phenomenon of proving credibility-for PTSD purposes- still prevails. If you were a 94B20 Cook, you would have to prove the gooks got in under the wire and overran the compound while you were there. VA accepts that everyone turns into an instant Eleven Bravo when that happens. VA uses the Joint Services Records Review Center (JSRRC) to do this. They have 12 (twelve-count ’em) “technicians” busy verifying your presence at LZ Bronco in 1968. Sometimes, this is impossible as many of you know. Everyone generally went to a dispersal depot and were assigned in country on an as-needed basis. These days, I use things like the Service treatment records (STRs) to show the APO zip code . You can access the list above https://asknod.org/vietnam-zip-codes/ to find most of them.

Lastly, the hoped-for gains at the BVA evaporated when the AMA swung into high gear. All of a sudden, a majority of Veterans decided screwing around down below at the Agency of Original Jurisdiction (AOJ) level was a dead end and decided the smart money was on a BVA decision. Unfortunately (you hear that word a lot at the VA), the AOJ was sloppy and a lot of claims that went to the BVA weren’t ready or had some defect like duty to assist or procedural error or ________________.

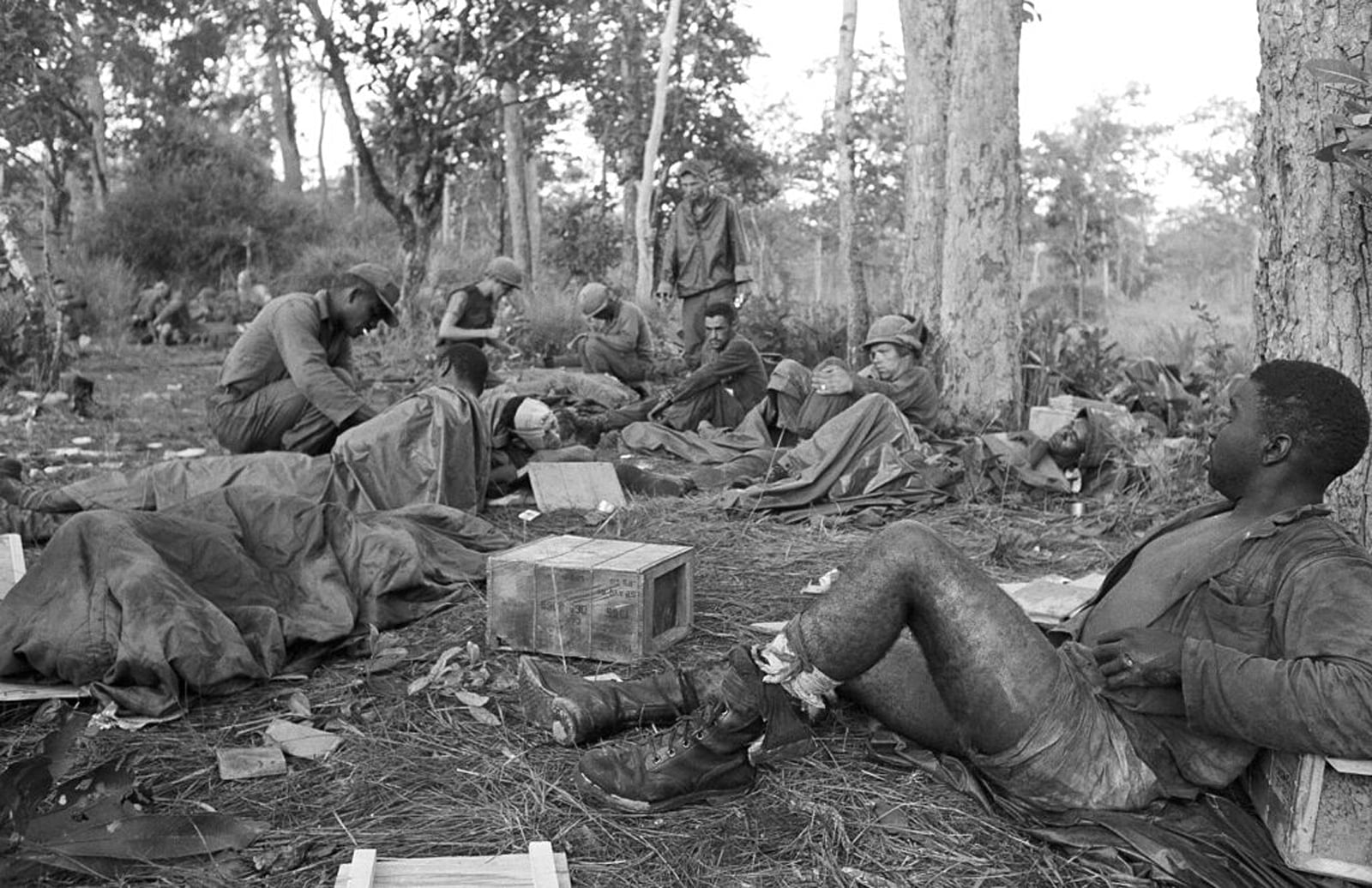
The BVA gomers weren’t having that. If the claim, now called a notice of disagreement (NOD) appeal, was not perfect, it got booted back to the AOJ (remanded) to be “fixed”. Even this didn’t help with the avalanche of NODs. The backlog at the BVA continues to defy the bean counters. In spite of hiring even more Veterans Law Judges (VLJs) the number of appeals continues to metastasize like an unruly cancer. Who woulda thunk it? We just engaged in nonstop war for twenty years and nobody saw this coming? Vietnam had a rather similarly sharp learning curve 50 or more years ago. It, too, persisted from 1961 to 1975 depending on who’s counting. VA Medical Centers couldn’t begin to hold them. Same old shit. Different day.

Since a lot of you read Veterans Help Websites looking for information on how to kick ass and take names, I think it’s only fair to point out a few problems I’m beginning to see. Most all of the “Elders” and Moderators of the web sites cut their teeth on the old Legacy System that existed prior to February 2019. The advice they offer is so far off the mark nowadays that it is deleterious to your claim or appeal. I honestly believe VSO Service Officers might be able to give you better advice. We need every asset we can muster. Newer Vets of the Iraquistan era need to inject new blood into these older sites to help their fellow Vets. One site I viewed recently is still offering advice on how to switch over to the RAMP system from Legacy. Newsflash. RAMP ended February 14, 2019. A frequent Moderator even proposed to offer advice on the VHA’s Caregiver program and baldly stated it would take two to five years to get a decision. Someone wise once said if you intend to preach, you better be well-acquainted with the Bible.

Different times call for different strategies in VAland. I used to advocate for HLRs before the Corona crisis. As of several months ago, I changed my mind. I’m batting about .300 on them now- and not for lack of finesse. The problem is simple. VA used to assign senior RVSRs or Quality Control RVSRs to these claims. As my practice has changed and focuses more on Special Monthly Compensation (SMC), I find that the HLR reviewers I get are GS 11s who are utterly clueless on the subject.

A good decision at the BVA is far more likely -but again, you have to pick wisely. You have three lanes from which to choose. The Direct or ‘no new evidence’ lane is the chicken dinner winner and here’s why. A request for a hearing will create a minimum of a two-year wait for a VLJ. Ditto for an evidence submission. I have several from 2020 still waiting. Worse, and a strong possibility due to the BVA gomers trying to pawn off as many as possible back to the AOJ, is the newer phenomenon of sending a dynamite IMO to the BVA and them kiting it back to the AOJ saying the AOJ deserves a shot at deciding if it’s a chicken dinner winner or a no-go. I leave it to you to guess the statistical outcome of those remands. Nothing like a fresh horse and a new rope for a VA Texas-style Necktie Party.

Get all your IMOs decided up or down at the AOJ. Submit and complete all the supplemental claims actions below. Make your BVA NOD Appeal rest entirely on the evidence of record. In more simple parlance, leave the VLJ with only one option-an up or down decision. Specify it in no uncertain terms. Tell them you’ll gladly waive any further review below and trust the VLJ to make the correct decision.
 One of these days we’ll see those Drive Thru claims systems in place. It’s just that I don’t have confidence it will happen in our time. And if any of you have discovered what use all of the items I mentioned above have, please by all means do share them with us.
One of these days we’ll see those Drive Thru claims systems in place. It’s just that I don’t have confidence it will happen in our time. And if any of you have discovered what use all of the items I mentioned above have, please by all means do share them with us.


P.S. Ed the LRRP sent this one in late.