
HCV METAVIR fibrosis staging: My old Marine suffered mightily when he was subjected to a “blind” (not ultrasound or CT guided) liver biopsy given by a resident at a teaching hospital. The resident had to make several passes to get a sample.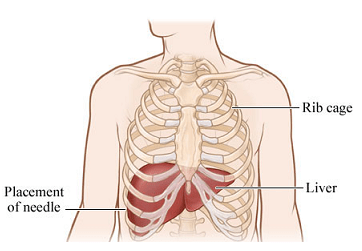
After 13 years of SVR status, the odds are good that he won’t need another liver puncture due to HCV. HCV residuals and HCV treatment (PEG-IFN-48 weeks) may require investigation in the future; because new technologies are being adapted, he need not suffer jabbing from another long fat biopsy needle.
The VA does not seem to promise veterans post-treatment cures or a lack of liver disease progression even if a patient achieves SVR. Patients are urged to take care of themselves, which is fine advice when they have the means and ability to do so.
The VA states (LINK to pdf): Achieving an SVR with HCV treatment improves clinical outcome. Liver fibrosis may improve (regress) after achieving an SVR. Patients with cirrhosis who achieve an SVR also have
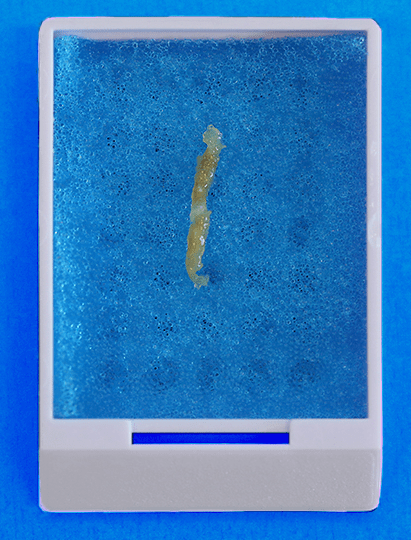
reduced progression of their liver disease and reduced risk of HCC, liver failure, and death related to liver disease, as well as reduced all-cause mortality.Image: The Royal College of Pathologists of Australasia
Liver biopsies, until recently, were considered the “gold standard,” but the VA and other medical establishments now appear to have downgraded their diagnostic usefulness. Now they aren’t even a silver or bronze standard.

VA HCV treatment advisory dated 10/18/17. Title: Chronic Hepatitis C (HCV) Infection: Treatment Considerations screenshot from page 45. Click image to read whole document.
VA advises their providers, “Liver biopsies may be considered but it is invasive and limited by potential sampling error.” I was pleased to see that the VA lists Magnetic Resonance elastography (MRE), invented by the Mayo Clinic (LINK), on their approved list.
Then and now
from VA Liver Fibrosis webpage (LINK)
Liver biopsy has been the gold standard for the assessment of histologic changes in the liver. In the past, liver biopsy was routinely performed in patients with HCV, particularly before HCV treatment…
…Requirements: If a biopsy is necessary, it should only be performed when the information will be useful for optimal patient care and cannot be obtained in another way. Furthermore, biopsy should only be performed after written informed consent has been obtained.

Liver biopsy sampling errors versus Magnetic Resonance Elastography (MRE) briefly explained in this short Mayo Clinic video. Click to view on Youtube.
The good news is that if gut problems arise again, one need not avoid going to the doctor due to fear of a painful needle biopsy.
The VA may be in the process of purchasing this technology but there are non-VA providers in certain areas of the country; DoD has one at Lackland AFB according to the map below. (The VA has invested in other noninvasive technologies.)
Mayo technical article (full text): MR elastography of liver disease: State of the art
For locations (LINK) and information (LINK).

I like the fact that Mayo Clinic and other researchers are studying MRE applications in breast, brain, and other parts of human anatomy. A safe, accurate MRE liver exam takes about 15 minutes. Takeaway? A state-of-the-art, painlessly derived visual map of the entire organ will result in better cheaper patient care. Call David (if he’s staying put–which the WaPo reports may not be the case).
Kiedove


I had them all! I like the new tech. the best. I still get tested every 6 months since my Transplant.
I noticed that Aetna’s private insurance won’t necessarily pay for the MREs, calling them experimental. They aren’t because they have been proven to be more accurate than punctures. I don’t know if Medicare is on-board yet. They should be because they are cost-effective. After a
liver biopsy, the patient is supposed to be observed for 2 hours for adverse effects–like bleeding, death….etc. A patient is supposed to live close to a hospital–just in case.
I’m excited about this technology also because many woman avoid mammograms out of fear of biopsies. It’s possible that this might be even better than the new 3D machines. And if early signs of dementias can be detected earlier, there are medications which can slow down disease progress. As with livers, the sooner a problem is detected, the faster treatment can begin and the better the outcome. Anyone with a history of HCV and/or exposure to AO (Camp Lejeune toxic water) needs to be aware of subtle changes that they might brush off as just being normal in an oldie.
3 for me, one hit so hard I almost jumped off the table, That s about the Time I started to hate the VA.
I assume your punctures weren’t “guided” (ex. ultrasound) either.
Hell no, the 1st one they had a guy training doing it with the doc standing there watching, he missed and Hit my rib, I almost jumped off the table, that one was done at Stanford, 2 more at VA and one from a real doctor.
This is the one I had done. With no anesthesia to boot.
Did you get a local at least–even though they are inadequate to combat the pain?
on the 1st one at Stanford, not at the VA, or the other doc.